
Primary Hyperparathyroidism
On this page:
- What is primary hyperparathyroidism?
- What do the parathyroid glands do?
- How common is primary hyperparathyroidism?
- Who is more likely to develop primary hyperparathyroidism?
- What are the complications of primary hyperparathyroidism?
- What are the symptoms of primary hyperparathyroidism?
- What causes primary hyperparathyroidism?
- How do doctors diagnose primary hyperparathyroidism?
- What tests do doctors use to look for complications of primary hyperparathyroidism?
- How do doctors treat primary hyperparathyroidism?
- Should I change my diet if I have primary hyperparathyroidism?
What is primary hyperparathyroidism?
Primary hyperparathyroidism is a disorder of the parathyroid glands, four pea-sized glands located on or near the thyroid gland in the neck. “Primary” means this disorder begins in the parathyroid glands, rather than resulting from another health problem such as kidney failure. In primary hyperparathyroidism, one or more of the parathyroid glands is overactive. As a result, the gland makes too much parathyroid hormone (PTH).
Too much PTH causes calcium levels in your blood to rise too high, which can lead to health problems such as bone thinning and kidney stones. Doctors usually catch primary hyperparathyroidism early through routine blood tests, before serious problems occur.
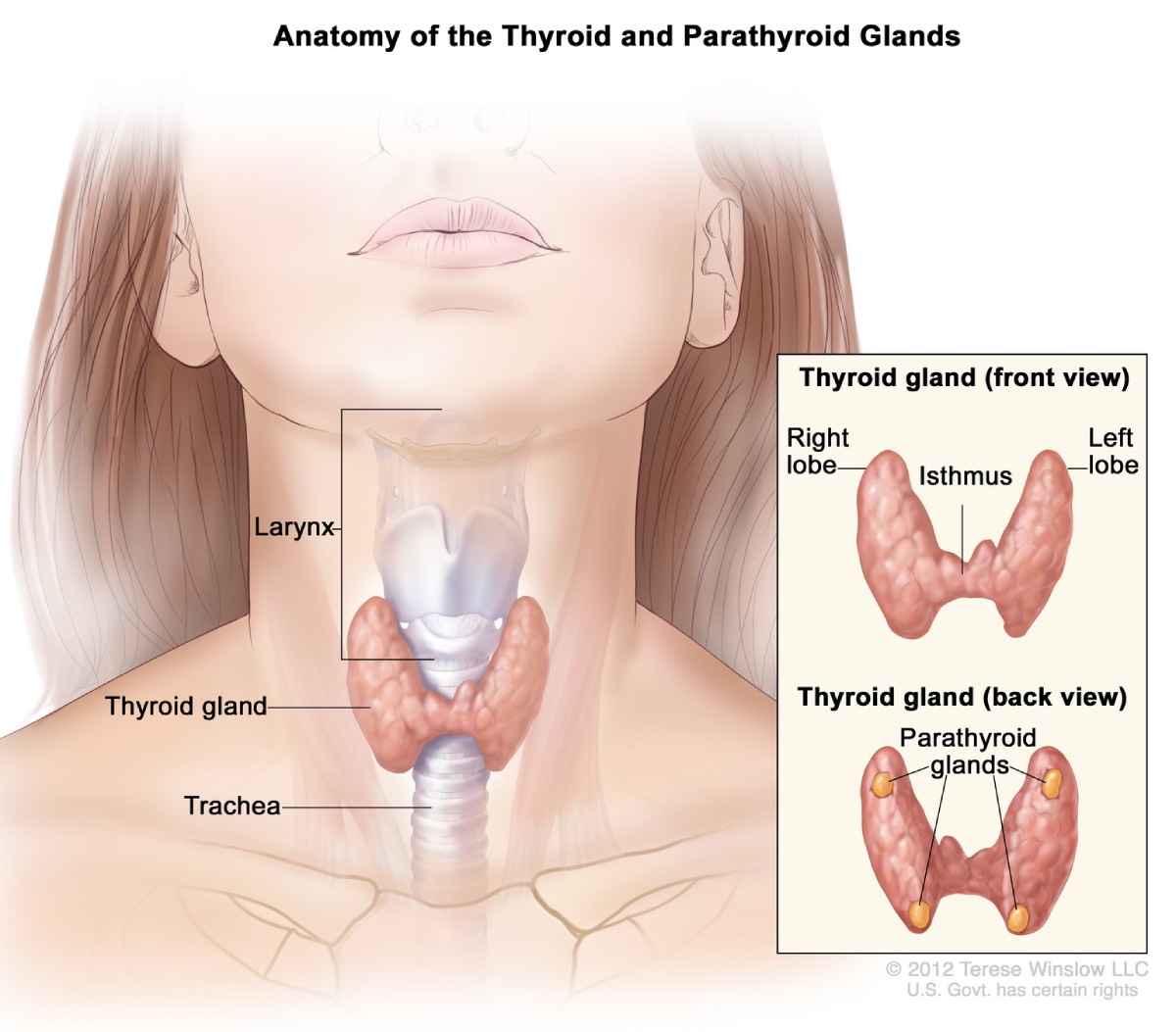 View full-sized imageThe parathyroid glands are located on or near the thyroid gland in the neck.
View full-sized imageThe parathyroid glands are located on or near the thyroid gland in the neck.
What do the parathyroid glands do?
The parathyroid glands’ only purpose is to make PTH, which helps maintain the right balance of calcium in your body. PTH raises blood calcium levels by
- causing bone, where most of your body’s calcium is stored, to release calcium into the blood
- helping your intestines absorb calcium from food
- helping your kidneys hold on to calcium and return it to your blood instead of flushing it out in urine
When the level of calcium in your blood falls too low, the parathyroid glands release just enough PTH to bring your blood calcium levels back to normal.
You need calcium for good health. This mineral helps build bones and teeth and keep them strong. Calcium also helps your heart, muscles, and nerves work normally.
Although their names are similar, the parathyroid glands and the thyroid gland are not related.
How common is primary hyperparathyroidism?
In the United States, about 100,000 people develop primary hyperparathyroidism each year.1 Primary hyperparathyroidism is one of the most common hormonal disorders.
Who is more likely to develop primary hyperparathyroidism?
Primary hyperparathyroidism most often affects people between age 50 and 60. Women are affected 3 to 4 times more often than men.1 The disorder was more common in African Americans, followed by Caucasians, in one large study performed in North America.1
What are the complications of primary hyperparathyroidism?
Primary hyperparathyroidism most often affects the bones and kidneys, although it also may play a part in other health problems.
Weakened bones
High PTH levels trigger the bones to release more calcium than normal into the blood. The loss of calcium from the bones may weaken them.
Kidney stones
The small intestine may absorb more calcium from food, adding to high levels of calcium in your blood. Extra calcium that isn’t used by your bones and muscles goes to your kidneys and is flushed out in urine. Too much calcium in your urine can cause kidney stones.
Other complications
High blood calcium levels might play a part in other problems, such as heart disease, high blood pressure, and trouble concentrating. However, more research is needed to better understand how primary hyperparathyroidism affects the heart, blood vessels, and brain.
What are the symptoms of primary hyperparathyroidism?
Most people with primary hyperparathyroidism have no symptoms. When symptoms appear, they’re often mild and similar to those of many other disorders. Symptoms include
- muscle weakness
- fatigue
- depression
- aches and pains in bones and joints
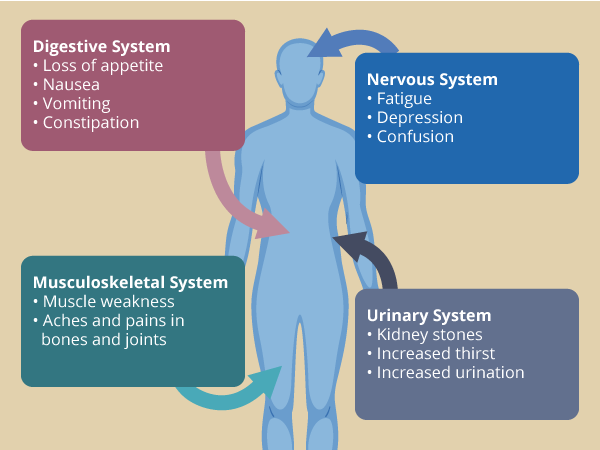 View full-sized imageSymptoms of primary hyperparathyroidism
View full-sized imageSymptoms of primary hyperparathyroidism
People with more severe disease may have
- loss of appetite
- nausea
- vomiting
- constipation
- confusion
- increased thirst and urination
What causes primary hyperparathyroidism?
In about 8 out of 10 people with primary hyperparathyroidism, a benign, or noncancerous, tumor called an adenoma has formed in one of the parathyroid glands.2 The tumor causes the gland to become overactive. In most other cases, extra PTH comes from two or more adenomas or from hyperplasia, a condition in which all four parathyroid glands are enlarged. People with rare inherited conditions that affect the parathyroid glands, such as multiple endocrine neoplasia type 1 or familial hypocalciuric hypercalcemia, are more likely to have more than one gland affected.
Rarely, primary hyperparathyroidism is caused by cancer of a parathyroid gland.
How do doctors diagnose primary hyperparathyroidism?
Doctors diagnose primary hyperparathyroidism when a blood test shows high blood calcium and PTH levels. Sometimes PTH levels are in the upper portion of the normal range, when they should drop to low-normal or below normal in response to high calcium levels. Other conditions can cause high calcium, but elevated PTH is the only source in primary hyperparathyroidism.
Routine blood tests can detect high blood calcium levels. High blood calcium may cause health care professionals to suspect hyperparathyroidism, even before symptoms appear.
Sometimes PTH levels are high but calcium levels are not. Doctors don’t routinely test for PTH but may do so if you have osteoporosis or another disorder that affects bone strength. In some cases, this may be the first phase of primary hyperparathyroidism, before calcium levels start to rise.
Once doctors diagnose hyperparathyroidism, a 24-hour urine collection can help find the cause. This test measures certain chemicals, such as calcium and creatinine, a waste product that healthy kidneys remove. You will collect your urine over a 24-hour period and your health care professional will send it to a lab for analysis. Results of the test may help tell primary hyperparathyroidism from hyperparathyroidism caused by a kidney disorder. The test can also rule out familial hypocalciuric hypercalcemia, a rare genetic disorder, as a cause.
What tests do doctors use to look for complications of primary hyperparathyroidism?
Once doctors diagnose primary hyperparathyroidism, they may use other tests to look for bone weakness, kidney problems, and low levels of vitamin D.
Bone mineral density test
Dual energy x-ray absorptiometry, also called a DXA or DEXA scan, uses low-dose x-rays to measure bone density. During the test, you will lie on a padded table while a technician moves the scanner over your body. A bone expert or radiologist will read the scan.
 During a DXA scan, you will lie on a padded table while a technician moves the scanner over your body.
During a DXA scan, you will lie on a padded table while a technician moves the scanner over your body.
Kidney imaging tests
Doctors may use one of the following imaging tests to look for kidney stones.
Ultrasound. Ultrasound uses a device called a transducer that bounces safe, painless sound waves off organs to create an image of their structure. A specially trained technician does the procedure. A radiologist reads the images, which can show kidney stones.
Abdominal x-ray. An abdominal x-ray is a picture of the abdomen that uses low levels of radiation and is recorded on film or on a computer. During an abdominal x-ray, you lie on a table or stand up. A technician positions the x-ray machine close to your abdomen and asks you to hold your breath so the picture won’t be blurry. A radiologist reads the x-ray, which can show the location of kidney stones in the urinary tract. Not all stones are visible on an abdominal x-ray.
Computed tomography (CT) scans. CT scans use a combination of x-rays and computer technology to create images of your urinary tract. CT scans sometimes use a contrast medium—a dye or other substance that makes structures inside your body easier to see. Contrast medium isn’t usually needed to see kidney stones. For the scan, you’ll lie on a table that slides into a tunnel-shaped machine that takes the x-rays. A radiologist reads the images, which can show the size and location of a kidney stone.
Vitamin D blood test
Health care professionals test for vitamin D levels because low levels are common in people with primary hyperparathyroidism. In patients with primary hyperparathyroidism, the low vitamin D level can further stimulate the parathyroid glands to make even more parathyroid hormone. Also, a very low vitamin D level may cause a secondary form of hyperparathyroidism, which resolves when vitamin D levels are returned to normal.
How do doctors treat primary hyperparathyroidism?
Guidelines help doctors to decide whether or not parathyroid surgery should be recommended. You might be a candidate for surgery if you meet any of these guidelines
- Blood calcium > 1 mg/dL above normal
- Bone density by DXA < -2.5 at any site (lumbar spine, hip, or forearm)
- History of kidney stones or evidence of kidney stones or calcifications in the kidney by imaging (e.g., X-ray, ultrasound, CT scan). Evidence for stone risk by 24-hour urine with excessive calcium and other stone risk factors.
- A fracture resulting from relatively little force, such as a fall from a standing or sitting position (a fragility fracture)
- Age < 50
Doctors most often recommend parathyroid surgery, particularly if the patient meets one or more of the guidelines noted above. It is also not inappropriate to recommend surgery in those who do not meet guidelines as long as there are no medical contraindications to surgery. In those who do not meet guidelines or do not choose surgery, the doctor will monitor the patient’s condition. If there is evidence for progressive disease (e.g., higher calcium level, lower bone density, a fracture, kidney stone), surgery would be advised. For patients who are not going to have parathyroid surgery, even though guidelines are met, doctors can prescribe medicines to control the high blood calcium or improve the bone density.
Surgery
Surgery to remove the overactive parathyroid gland or glands is the only sure way to cure primary hyperparathyroidism. Doctors recommend surgery for people with clear symptoms or complications of the disease. In people without symptoms, doctors follow the above guidelines to identify who might benefit from parathyroid surgery.2 Surgery can lead to improved bone density and can lower the chance of forming kidney stones.
When performed by experienced surgeons, surgery almost always cures primary hyperparathyroidism.
Surgeons often use imaging tests before surgery to locate the overactive gland or glands to be removed. The tests used most often are sestamibi, ultrasound, and CT scans. In a sestamibi scan, you will get an injection, or shot, of a small amount of radioactive dye in your vein. The overactive parathyroid gland or glands then absorb the dye. The surgeon can see where the dye has been absorbed by using a special camera.
Surgeons use two main types of operations to remove the overactive gland or glands.
Minimally invasive parathyroidectomy. Also called focused parathyroidectomy, surgeons use this type of surgery when they think only one of the parathyroid glands is overactive. Guided by a tumor-imaging test, your surgeon will make a small incision, or cut, in your neck to remove the gland. The small incision means you will probably have less pain and a faster recovery than people who have more invasive surgery. You can go home the same day. Your doctor may use regional or general anesthesia during the surgery.
Bilateral neck exploration. This type of surgery uses a larger incision that lets the surgeon find and look at all four parathyroid glands and remove the overactive ones. If you have bilateral neck exploration, you will probably have general anesthesia and may need to stay in the hospital overnight.
 When performed by experienced surgeons, surgery almost always cures primary hyperparathyroidism.
When performed by experienced surgeons, surgery almost always cures primary hyperparathyroidism.
Parathyroid surgery is safe. Rarely, problems can occur after surgery. In about 1 out of every 100 people, the nerves controlling the vocal cords are damaged during surgery, which most often results in hoarseness.3 This condition usually gets better on its own.
Low calcium levels in the blood may occur after surgery but usually return to normal in a few days or weeks. On rare occasions, not enough parathyroid tissue is left to make PTH, which can result in hypoparathyroidism.
Monitoring
Some people who have mild primary hyperparathyroidism may not need surgery right away, or even any surgery, and can be safely monitored.
You may want to talk with your doctor about long-term monitoring if you
- don’t have symptoms
- have only slightly high blood calcium levels
- have normal kidneys and bone density
Long-term monitoring should include regular doctor visits, a yearly blood test to measure calcium levels and check your kidney function, and a bone density test every 1 to 2 years.
If you and your doctor choose long-term monitoring, you should
- drink plenty of water so you don’t get dehydrated
- get regular physical activity to help keep your bones strong
- avoid certain diuretics, such as thiazides
Medicines
Cinacalcet is a medicine that decreases the amount of PTH the parathyroid glands make and lowers calcium levels in the blood. Doctors may prescribe cinacalcet to treat very high calcium levels in people with primary hyperparathyroidism who can’t have surgery.
Cinacalcet does not improve bone density. If you have bone loss, your doctor may prescribe alendronate or other medications to help increase bone density.
Should I change my diet if I have primary hyperparathyroidism?
You don’t need to change your diet or limit the amount of calcium you get from food and beverages. You will need to take a vitamin D supplement if your vitamin D levels are low. Talk with your health care professional about how much vitamin D you should take.
If you lose all your healthy parathyroid tissue and develop lasting low-calcium levels, you’ll need to take both calcium and vitamin D for life.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
John P. Bilezikian, M.D., Columbia University