What are aplastic anemia and myelodysplastic syndromes (MDS)?
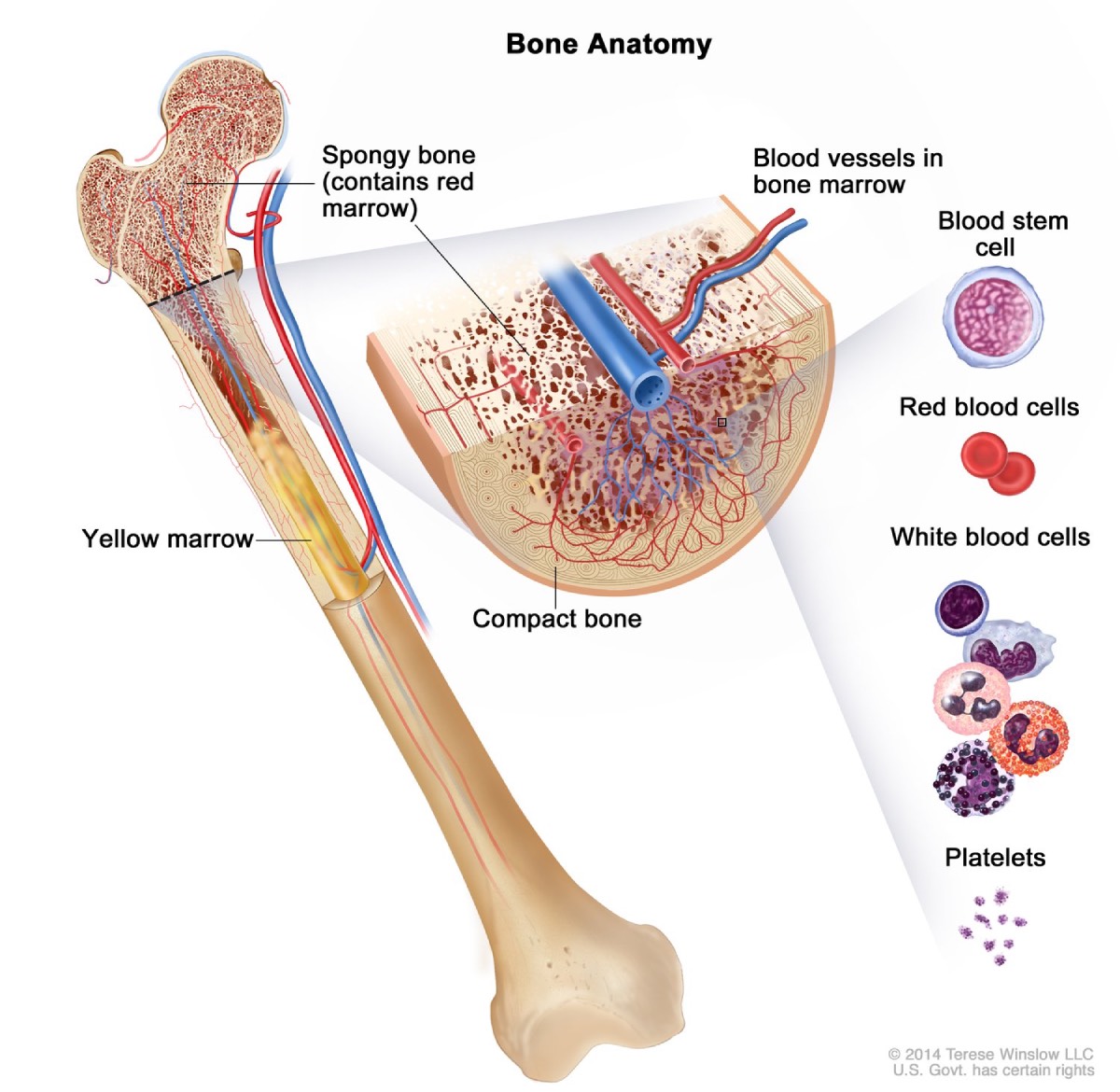
Aplastic anemia and myelodysplastic syndromes (MDS) are rare but serious disorders that affect bone marrow and blood. Bone marrow is the soft, sponge-like tissue inside your bones. Your bone marrow contains blood stem cells, which make of all the red blood cells, white blood cells, and platelets carried around in your blood. In both aplastic anemia and MDS, your bone marrow is injured and doesn’t produce enough healthy blood cells, which leads to lower than normal levels of at least two of the three blood cell types.
Each of the three types of blood cells—all made in the bone marrow—performs an important job.
Red blood cells contain hemoglobin, which is a protein that carries oxygen from your lungs to all parts of your body. Having fewer red blood cells than normal is called anemia.
White blood cells are an important part of your immune system, helping your body fight infections. Having fewer white blood cells than normal is called leukopenia.
Platelets are small blood cells that stick together to stop bleeding and help wounds heal. Having fewer platelets than normal is called thrombocytopenia.
In aplastic anemia, many of your bone marrow’s stem cells are injured or destroyed. With fewer stem cells, your bone marrow cannot produce an adequate number of blood cells, though the cells that are produced are healthy. In MDS, some of your bone marrow’s stem cells are damaged and produce unhealthy blood cells that do not work properly, leaving you without enough working, mature blood cells.
View full-sized imageAll three types of blood cells—red blood cells, white blood cells, and platelets—develop from blood stem cells in the bone marrow.
Are there other names for aplastic anemia and MDS?
Aplastic anemia and MDS are types of bone marrow failure. MDS is sometimes called myelodysplasia or preleukemia.
How common are aplastic anemia and MDS?
Aplastic anemia is rare. About 2 out of every 1 million people in the United States are diagnosed with aplastic anemia each year.1
Myelodysplastic syndromes are also rare, especially in people younger than age 60. The risk of developing MDS increases as people age, so the total number of MDS cases is likely to grow as the U.S. population ages.2
Who is more likely to develop aplastic anemia or MDS?
Aplastic anemia
Aplastic anemia can affect people of any age, but it’s more likely to develop between the ages of 2 to 5, 20 to 25, and 55 and older.3 The disorder affects men and women equally.1
Your risk of developing aplastic anemia is higher with1
MDS can occur at any age, but your risk for developing the disease increases as you get older. The disorder is most common in people ages 60 and older, and it affects men about twice as often as women.4
Your risk for MDS is higher with5
long-term exposure to certain chemicals, including benzene, pesticides, and tobacco
What are the complications of aplastic anemia and MDS?
Aplastic anemia and MDS can be life-threatening. Too few healthy red blood cells can lead to severe anemia and heart failure because your body isn’t getting enough oxygen. When your body doesn’t make enough healthy white blood cells, you are at risk of developing severe infections. Without enough healthy platelets, you can experience spontaneous internal bleeding.
People with aplastic anemia or especially MDS are at greater risk of developing acute myeloid leukemia, a blood cancer that affects the bone marrow.
References
Symptoms & Causes
What are the symptoms of aplastic anemia and MDS?
The symptoms of aplastic anemia and MDS are very similar. Symptoms of the disorders may include
fatigue or tiredness
frequent infections
unexplained or easy bruising
nosebleeds, bleeding gums, or any bleeding that lasts too long
unusually pale skin
weakness
shortness of breath when exercising or being active
red or purple spots on the skin caused by bleeding under the skin
fast or irregular heartbeat
dizziness
fever
headache
Symptoms vary from person to person, depending on which type of blood cells are most affected and the cause of the disorder. In the early stages of MDS, you may have only mild symptoms or no symptoms at all.
Fatigue can be a symptom of aplastic anemia, MDS, and many other disorders. Medical tests may help find the cause of your tiredness.
Seek care right away
If you have a fever or bleeding that won’t stop, contact your health care professional right away. Ask your health care professional what other symptoms may need quick care. Severe aplastic anemia and higher-risk MDS, which occur when you have very low levels of one or more types of blood cells, can be life-threatening if not treated right away.
What causes aplastic anemia and MDS?
Aplastic anemia
In most cases, the exact cause of aplastic anemia is not known. This is called idiopathic. However, researchers believe that the disorder may result from the body’s own immune system causing damage to bone marrow stem cells. Certain environmental or health conditions are also associated with aplastic anemia and can trigger the disorder.
Aplastic anemia can be acquired, meaning it develops after birth, or it can be inherited, meaning it is passed down in genes from your parents. Acquired aplastic anemia is more common than the inherited disorder. With inherited aplastic anemia, it’s important that siblings also be tested for the disease so that it can be treated as early as possible.
MDS
Most cases of MDS are linked to changes to the DNA in stem cells in the bone marrow, but the exact cause is usually not known. Aging may play a role, because as you age your stem cells get older and are more likely to develop abnormalities that can lead to MDS. Certain environmental or health conditions, such as radiation and chemotherapy treatment, exposure to certain chemicals, and smoking are also associated with MDS.
Diagnosis
How do health care professionals diagnose aplastic anemia and MDS?
Your health care professional will use your medical and family history, physical exam, and test results to diagnose your condition. Your health care professional may refer you to a hematologist, a doctor who treats blood disorders, or an oncologist, a doctor who treats cancer.
What tests do health care professionals use to diagnose aplastic anemia and MDS?
Blood tests
Your health care professional may use one or more blood tests to check for signs of aplastic anemia or MDS.
A complete blood count, or CBC, is usually the first blood test used to check for aplastic anemia or MDS. The test measures hematocrit, which is the portion of the blood sample made up of red blood cells. A CBC also measures
the amount of hemoglobin, a protein in your red blood cells that carries oxygen to your body
the number of red blood cells and platelets
the number and types of white blood cells
A blood smear examines the size, shape, and number of blood cells in your blood.
Health care professionals sometimes use blood tests to check for unusual amounts of folate, vitamin B12, and erythropoietin—a hormone made by your kidneys to help produce red blood cells.
A complete blood count is usually the first test your health care professional will use to check for aplastic anemia or MDS.
Your health care professional may order other specialized tests to help find the cause of your aplastic anemia or MDS or to identify other disorders you may have. Other tests your care team may order include
flow cytometry, which measures the number of cells, percentage of live cells, and certain characteristics of cells such as size and shape
molecular testing, which checks for abnormal changes in specific genes
How do health care professionals treat aplastic anemia?
Health care professionals treat aplastic anemia by first treating any underlying condition that might be triggering the aplastic anemia, if an underlying condition is suspected. This may include removing exposure to a chemical, stopping a certain medicine, or treating a viral infection.
Your care team may recommend one or more of the following treatment options
blood transfusion
bone marrow stem-cell transplants
immunosuppressive therapy
medicines
Treatments for aplastic anemia can ease your symptoms, improve your quality of life, and, in some cases, provide a cure for the disorder. Your treatment will depend on your age, general health, cause and severity of the disease, and availability of a stem-cell donor. Mild or moderate aplastic anemia may not need immediate treatment.
Blood transfusions
Blood transfusions can temporarily relieve symptoms such as anemia, fatigue, and bleeding by increasing the amount of red blood cells or platelets or both in your blood.
Repeat transfusions are common but can lead to other health problems.
Iron from transfused red blood cells can build up in the body and damage organs, called iron overload or hemochromatosis. Your health care professional can prescribe treatments that remove extra iron.
Over time, the body may develop antibodies that damage or destroy the donor blood cells. Your health care professional may prescribe medicines to prevent or manage this reaction.
Blood and bone marrow stem-cell transplants
Blood and bone marrow transplant, also called a stem-cell transplant, uses a donor’s healthy stem cells to replace your body’s own damaged stem cells. The donor’s cells must closely match yours for the best outcomes. Close relatives such as siblings are more likely to be close matches, but unrelated donors can also be close matches. If a matched donor isn’t found in your family, your doctor will search the National Marrow Donor Program, which has millions of potential donors.
Stem-cell transplant is the only possible cure for aplastic anemia. Talk with your health care professional about the risk and benefits of a stem-cell transplant and if the procedure is right for you.
Immunosuppressive therapy
Immunosuppressive therapy may be used for people who cannot have a stem-cell transplant or to control aplastic anemia in people who are waiting for a stem-cell transplant. Immunosuppressants, such as antithymocyte globulin (ATG) and cyclosporine, suppress your body’s immune system and slow or stop damage to your bone marrow. This is not a cure though. Your health care professional may use a medicine called eltrombopag in combination with an immunosuppressant to increase the number of blood cells in your body.
Medicines
Low white blood cell counts can make it hard for your body to fight off infections. Your care team may give you medicine to kill bacteria, fungi, or viruses that cause infection.
How do health care professionals treat MDS?
Treatment for MDS is similar to treatment for aplastic anemia. However, because most people with MDS are older adults and may have other health problems, treatment for MDS focuses on supportive care to ease your symptoms, improve your quality of life, and prevent bleeding and infections rather than curing the condition. Some people live for many years with supportive care alone.
People who have few or no symptoms may not need treatment. If you develop symptoms, have worsening symptoms, or have very low blood cell counts, treatment will be tailored to your age, general health, symptoms, and cause and severity of the disease. A stem-cell transplant may offer a chance for a cure for certain people.
Blood transfusions
Blood transfusions increase the number of healthy red blood cells or platelets in your body. You may need a transfusion occasionally or possibly as often as every week or two.
Medicines
Medicines to stimulate bone marrow. Medicines called growth factors may ease your symptoms by helping your bone marrow make more blood cells. These medicines are copies of substances found naturally in your body, such as erythropoietin and granulocyte colony-stimulating factor.
Medicines to treat or prevent infections. Fewer white blood cells make it harder for your body to fight infections. Antibiotics may be used to kill bacteria that cause infections.
Hypomethylating agents. Medicines that help prevent the growth of abnormal bone marrow stem cells and increase the number of healthy blood cells in your body may improve your quality of life and lower your chances of developing leukemia. Your health care professional may ask you to take a hypomethylating agent such as azacitidine or decitabine.
Immune modulators. Your health care professional may prescribe the immune modulator lenalidomide to slow the growth of abnormal blood cells and lessen your need for blood transfusions.
Immunosuppressive therapy
In some people with cases of MDS that are thought to be more similar to aplastic anemia, medicines that calm the body’s immune system can slow or stop damage to bone marrow. These immunosuppressant medicines, including ATG and cyclosporin, may relieve your symptoms and help you avoid blood transfusions.
Blood and bone marrow stem-cell transplants and chemotherapy
Stem-cell transplant and chemotherapy medicine can be used separately or together to treat MDS. These treatments are more aggressive and may improve blood counts more quickly than less intensive treatments, reduce the risk of death from MDS, and possibly provide a cure. But these treatments have greater risks of complications so they are used in patients in whom the risk and benefits have been clearly assessed.
For people with more advanced MDS or those at greater risk of developing acute myeloid leukemia, your care team may prescribe traditional chemotherapy medicine to help your body get rid of the abnormal cells. Traditional chemotherapy medicines include cytarabine, daunorubicin, and idarubicin. This treatment may be too toxic for some older people or those with other health problems.
Treatments for aplastic anemia and MDS depend on how severe the disorder is, your age, and other factors. Talk with your health care professional about the treatment options that might be best for you.
Eating, Diet, & Nutrition
How can my diet help prevent or relieve aplastic anemia and MDS?
Eating, diet, and nutrition have not been shown to play a role in preventing or treating aplastic anemia and MDS. However, people with either disorder who receive a stem-cell transplant need to eat a healthy diet to help with their recovery. You may need to avoid some foods too, to lower the chances of infection while your immune system is still weak after a transplant. Ask your health care professional for guidelines.
People with low white blood cell counts are at risk for infections and should follow food safety guidelines for people with cancer, which include
fully cook all meat, fish, and egg dishes
avoid fruits and vegetables that you cannot peel
avoid raw foods
avoid unpasteurized cheese, milk, and other dairy products
avoid unpasteurized juices
Clinical Trials
The NIDDK conducts and supports clinical trials in many diseases and conditions, including blood diseases. The trials look to find new ways to prevent, detect, or treat disease and improve quality of life.
What are clinical trials for aplastic anemia and MDS?
Clinical trials—and other types of clinical studies—are part of medical research and involve people like you. When you volunteer to take part in a clinical study, you help doctors and researchers learn more about disease and improve health care for people in the future.
Researchers are studying many aspects of aplastic anemia and MDS, such as
the efficacy of new combination treatments
new methods of stem-cell transplant to reduce complications and improve outcomes
optimal dose of immunosuppressants following stem-cell transplant
Watch a video of NIDDK Director Dr. Griffin P. Rodgers explaining the importance of participating in clinical trials.
What clinical studies for aplastic anemia and MDS are looking for participants?
You can view a filtered list of clinical studies on aplastic anemia and MDS that are federally funded, open, and recruiting at www.ClinicalTrials.gov. You can expand or narrow the list to include clinical studies from industry, universities, and individuals; however, the NIH does not review these studies and cannot ensure they are safe. Always talk with your health care provider before you participate in a clinical study.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Amy E. DeZern, M.D., M.H.S., Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, The Johns Hopkins University School of Medicine