


How Can Pharmacists Help Patients Improve Medication Adherence?

Pharmacists can play an important role in helping patients with diabetes understand their medications and take them as prescribed.
In this third interview of a three-part series on medication adherence, Candis M. Morello, PharmD, APh, CDCES, FCSHP, FASHP, identifies services that pharmacists can offer patients with diabetes to improve their medication adherence to avoid serious health complications and higher health care costs.
Q: What does medication adherence mean for patients with diabetes and their health care professionals?
A: The definition of medication adherence can be a little different for patients versus health care professionals. For patients, sometimes it’s observed as, “The doctor’s telling me I have to take these medications, but I already take 12 or more.” It can be overwhelming. And they think, “Maybe if I forget to take them or if I miss a few days, it’s not a big deal.” Whereas for health care professionals, medication adherence means taking medications correctly, just as they were prescribed, and making sure it’s the right drug and dose, and the right timing, frequency, and method of administration. Getting the patient and the health care professional on the same page is necessary.
It’s hard sometimes for patients to realize the importance of medication adherence, because they might have type 2 diabetes for years until they actually start to exhibit symptoms. So, when you’re not feeling anything negative, sometimes it’s hard to understand why you need to take the medicines. However, I am 100% positive that there are interventions that we as clinical pharmacists can employ to help patients achieve glycemic control through better adherence.
Q: What factors affect whether people with diabetes adhere to their prescribed medication therapy?
A: It’s helping patients, listening to them, and figuring out what the barriers are. “Why are you having trouble remembering to take your medications?” “Is the medication regimen too complex?” “Do you have too many medicines?” “Is the timing of the medication something that you just can’t remember?” It could be that their diabetes has not been managed for so long that they just fall asleep before taking the medication.
It’s not always just one thing. There can be a high-cost burden associated with medications, particularly some of the newer agents, and there are other socioeconomic issues as well.
Patients don’t always feel like they have been heard. Or they’ve been listened to, but the response they received was, “Here, take another medicine.” So, I’m very big on sitting down with the patient to hear what is happening with them. Then usually, very quickly, I can figure out what the barriers and motivating factors are to help them want to adhere to their medicine regimen.
Symptoms can be incentives to take medicines as prescribed, too. For example, if a patient has microalbuminuria or mild nonproliferative diabetic retinopathy, we can say, “Don’t worry. All we have to do is get your diabetes under control so that the condition either does not progress, or we can reverse it.” Having to get up at night due to nocturia, getting only two or three hours of sleep at a time because you need to urinate, is exhausting, especially for my patients who are homeless and have to climb out of a warm sleeping bag when it’s cold outside. I get a lot of new consults for men who have erectile dysfunction, and they realize it’s the diabetes. I tell them, “Let’s help you manage your diabetes. We can fix this.” They’re very compliant!
Q: What are some of the ways that pharmacists can help patients adhere to their medication regimen?
A: Pharmacists can have a significantly positive impact on patient medication adherence by performing medication reconciliation, which means reviewing all of the patient’s medicines and identifying realistic solutions to their adherence issues.
This could be, for example, simplifying their regimen as much as possible to once- or twice-daily medication times that are paired with some other activity, or reducing the regimen complexity by changing the medicine to lower the number of injections needed per month. We’ve been very fortunate in the last decade to have the emergence of new drugs and medication classes that have come out to help our patients achieve their glycemic goal with more simplified regimens.
Some of my patients say that they forget to take their medicines three or four times a week, because they go to work without taking their pills with them. So, we recommend a pill box to keep at work or in their backpack or purse. There are multiple other suggestions that pharmacists might offer, such as to put reminders in patients’ phones or to use a phone app that helps with medication adherence.
Pharmacists also can help with patient assistance programs, helping patients get medicines at a better price or recompensated through drug company programs.
Q: You have developed some visual aids for educating patients. Can you describe them?
A: I find that my patients really resonate with visuals. I use a spiderweb visual. I say to my patients, “This diabetes is complex, so I’m going to ask you a lot of questions to get to know you, then tell you things we have to offer, and you can make the choices.” This sets the stage so they understand why I’m asking all these personal questions.
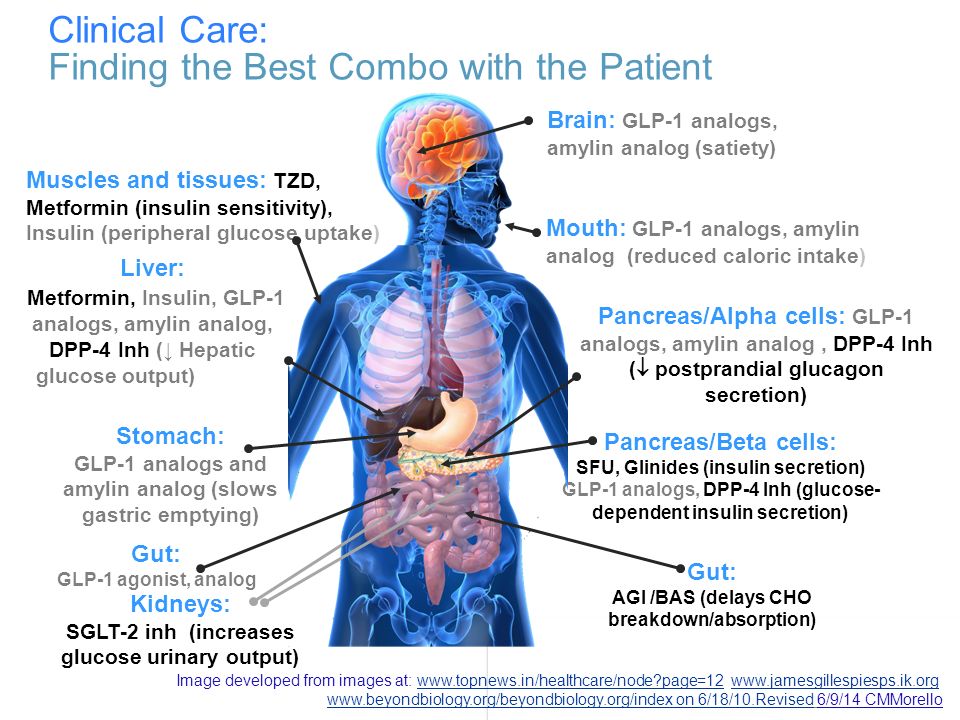
I also show them a picture of the body, and I have each medicine listed near the organ where it works. I say, “This is the reason why you’re on this medicine, and this medicine. They target different areas to work together to help your body achieve glycemic control.” And then patients get it.
{kind=link}
I was also having a hard time getting patients to understand what the blood glucose numbers they tested meant and how those values impacted the body, so I created another visual. On an X-axis, there’s time of day, and on the Y-axis is the glucose value. I created color-coded zones, with grey for 80 and below, red for 131 and above, and yellow for the zone in between that we’re trying to target, which for most patients it’s 80 to 130. The red zone with blood glucose values of 131 to 400 has pictures of the eyes, the kidneys, the nerves, the heart, and the brain to show that when the glucose values are that high at any time of day, it impacts those organs.
We look at this at their first visit, and again in 3 months, to see where they are in the zones. Patients like it; they see their progress and ask to take it home and put it on their refrigerator!
Q: What is the pharmacist’s role when a person comes into the pharmacy with signs of undiagnosed diabetes?
A: Sometimes people will come into a pharmacy with a yeast infection that keeps occurring over and over, or they want an over-the-counter medicine because they have to get up and go to the bathroom several times at night. If you’ve asked questions to narrow down the cause and rule out other possibilities, you can say, “Sometimes, this is associated with elevated glucose concentrations, and I really think it might be important that you go in and get tested by your doctor. When’s your next primary care doctor appointment?”
Q: Some pharmacists offer medication adherence clinics. What are they?
A: These clinics are very effective for pharmacists to work collaboratively with other members of the health care team. Where I work, patients are usually referred by a primary care provider to the medication adherence clinic. These are patients that need more time to go over medications and adherence in more detail than the primary care provider can provide in a typical appointment.
I have a memorandum of understanding with an endocrinologist that I work under, with an approved scope of practice. This provides me with prescribing privileges in my clinic for the patient’s diabetes care. I can initiate, adjust, and discontinue any medicine; titrate; order labs; and do anything that needs to be done within the scope of diabetes and comorbid conditions.
Basically, what we’re doing at this clinic is looking at the patient’s medicines. Are they the correct drug and dose frequency, and is the patient taking the medicine? One way we can tell that is based on the refill rate.
One of the things that we do is identify the motivating factors for the patient. We ask questions to narrow that down, because not everybody has the same motivating factor. Some people aren’t motivated to avoid long-term complications, but they care about family. It could be they have a parent to care for, or they want to live to see their granddaughter’s graduation.
My clinic is a tune-up for patients, where we provided multimodal personalized care. We’ve looked to see how they do after they leave the clinic, up to 12 months later. And guess what? Their glucose management did not get worse. It starts to wane a little bit around the 9-month mark, but you can bring them back to the clinic for a quick touchpoint somewhere around that time.
Q: What’s the evidence that educating patients about medication adherence is effective?
A: If we educate patients with diabetes—not make any medication changes, but just educate—we can reduce A1C by 0.5% or so, and then their usual care will add another 1% reduction in A1C. We have demonstrated long-term outcomes of up to a 3% reduction in A1C levels with the tune-up clinic method.
Q: How can health care professionals find pharmacists who can help their patients with diabetes better manage their medicines?
A: In hospital or ambulatory care settings, health care professionals can refer their patients to onsite clinics managed by pharmacists. The pharmacists can bill for medication therapy management services.
Health care professionals can also encourage patients to develop a relationship with their local pharmacist. Pharmacies are in communities everywhere, and they have trained pharmacists with the skills to help patients better manage their medications. Even if a pharmacist doesn’t have a memorandum of understanding with a customer’s primary health care professional, it just takes a call to the provider to make a suggestion for a medication adjustment that might benefit the patient’s adherence.
There are many pharmacists in the United States who have the Certified Diabetes Care and Education Specialist (CDCES) credential. The Association of Diabetes Care & Education Specialists offers a national registry of everyone with that credential.