


Addressing Depression and Suicide Risk in Patients with Diabetes

Learn why screening for depression and suicidal thoughts is an important part of diabetes care.
The daily burdens that people with diabetes deal with may increase their risk for depression and suicide. Shideh Majidi, MD, MSCS, explains why diabetes health care professionals should screen patients for depression and suicide risk and have a plan for helping patients who screen positive.
Q: How can having diabetes affect a patient’s mental health?
A: Type 1 and type 2 diabetes are both chronic illnesses, and we know that kids and adults who have chronic illnesses are more likely to have depression and anxiety.
Because diabetes is pretty much a 24/7 disease, patients think about it all the time. What they’re eating, how much they’re eating, what activity they are doing—that kind of day in, day out burden can increase the risk for both depression and anxiety. People also experience diabetes distress, which is related to the burden of having diabetes and has been associated with depression as well.
While there isn’t conclusive information yet, there are also some questions about whether changes in the brain occur when you have depression that can affect diabetes, and vice versa.
Q: Does technology for diabetes management relieve the mental health burden or add to it?
A: For some people, technology can definitely help decrease the burden. For example, insulin pumps can help them fine-tune their dosing and manage their blood glucose. The pumps partially do this in the background, especially these new hybrid closed-loop pumps, although the person still has to do work in terms of bolusing, that is, giving themselves doses of insulin through the pump as needed.
However, these tools sometimes can be a burden. For example, I work with children, and we start continuous glucose monitors (CGMs) at diagnosis or close to diagnosis. For some patients and their families, if you give them a CGM that tells them their blood glucose or their child’s blood glucose all the time and they’re seeing the rises and the drops, then that can cause more stress. But in other cases, it gives patients and their families relief because they can see what’s going on. So, it depends on the situation and the person.
Q: How does the risk of suicide compare for people with and without diabetes?
A: Suicidal ideation is reported by about 8% to 15% of children who have type 1 diabetes, with a similar percentage for adults with diabetes. Some reviews note that the risk of suicide is up to twice as high in type 1 and type 2 diabetes compared to the general population. True levels are not known because it is likely that cases of suicide from diabetes are underreported.
Let’s say a person dies from a hypoglycemic seizure. Is it because they unintentionally had a seizure or because they intentionally gave themselves too much insulin? Insulin can be both a life-saving and life-threatening medication. In patients with type 1 and in some patients with type 2, you need insulin to survive. But at the same time, insulin can be manipulated as a form of self-harm or to attempt suicide.
Q: Why is it important to screen patients with diabetes for depression and suicide risk?
A: When we see a patient who may be struggling with their diabetes, we can talk to them as much as we want about checking blood glucose more, making sure they have their CGM on, making sure they’re bolusing. But if they have depression and don’t have the energy, the ability, or even the want to do those things, then we’re not addressing the problem. Knowing that the patient has depressive symptoms or depression and helping them manage that ultimately will help in managing the diabetes as well. The American Diabetes Association Standards of Care and the International Society for Pediatric and Adolescent Diabetes Clinical Practice Consensus Guidelines both recommend routine screening of youth and adults for mental health disorders such as depression.
Q: Does asking people if they have suicidal thoughts put the idea in their head?
A: That is definitely a worry that health care professionals can have. But what happens is really the opposite. If patients are thinking about it, they’re thinking about it; us asking is not going to implant anything in their mind. Rather, asking about suicidality lets them know that we are there for them and we want to help them. So, it actually can be very helpful to ask that question, because then patients feel like they have somebody they can talk with about what is going on.
Q: How can a clinical practice screen for depression and suicide risk and follow up with patients?
A: The workflow should include screening for depressive symptoms and a follow-up risk assessment for those who screen positive for suicidal ideation. The biggest thing to start with is using a depression screener that has a question that specifically asks about suicidality, such as the Patient Health Questionnaire-9 (PDF, 723 KB).
If a patient expresses suicidal ideation, the follow-up is a suicide risk assessment, such as the Columbia Suicide Severity Rating Scale (C-SSRS) (PDF, 186 KB). How acute is the situation? Have they attempted before? Do they have a plan? That really helps to reveal whether it’s a situation where we need to send somebody to the emergency room, or where they’re having these thoughts but they’re not currently at acute risk and we can do things that can help prevent them from getting to that acute stage.
In terms of depression, it’s important to have the follow-up in place to provide patients with resources, such as a referral to a behavioral health specialist.
I think it is very helpful to have behavioral health specialists—social workers or psychologists—as part of your diabetes care team. They can not only screen for mental health disorders, but also treat and work with families to help manage and even prevent mental health disorders with early screening.
There are a couple of great resources. One is the RESCUE Collaborative Community, which is trying to educate health care practices across the globe about how they can implement screening to reduce suicide attempts. There’s also the Type 1 Diabetes Exchange Quality Improvement Collaborative. It provides documentation from different centers on how they have implemented depression screening.
Q: What guidance do you have for health care professionals to help patients who have suicidal thoughts but are not at acute risk for suicide?
A: Sometimes a person screens positive, but when you do the risk assessment, you learn that they’re not really talking about wanting to kill themselves. For example, I’ve had a couple of patients tell me, “If I don’t take care of my diabetes, I’m going to get all these complications, which means that I’m going to die, so of course, I think about dying all the time.” That’s definitely different than wanting to kill yourself.
When you find that the suicide risk is not acute, then you can review positive coping strategies—things the individual can do when they have thoughts of hurting or killing themselves that can help take them away from those thoughts. For a child or young adult, I like to have on that list an adult they feel comfortable talking with. For all patients, there should also be the number for the suicide hotline. If they get through their list and they’re still having those thoughts, then it’s important for them to have the numbers of professionals they can call.
If you make a list, the patient can either take a picture of it or keep it with them in their wallet. When a patient is in that frame of mind, it is hard to know what to do. It can be really helpful to have something they can look at and say, “This is my coping strategy plan.”
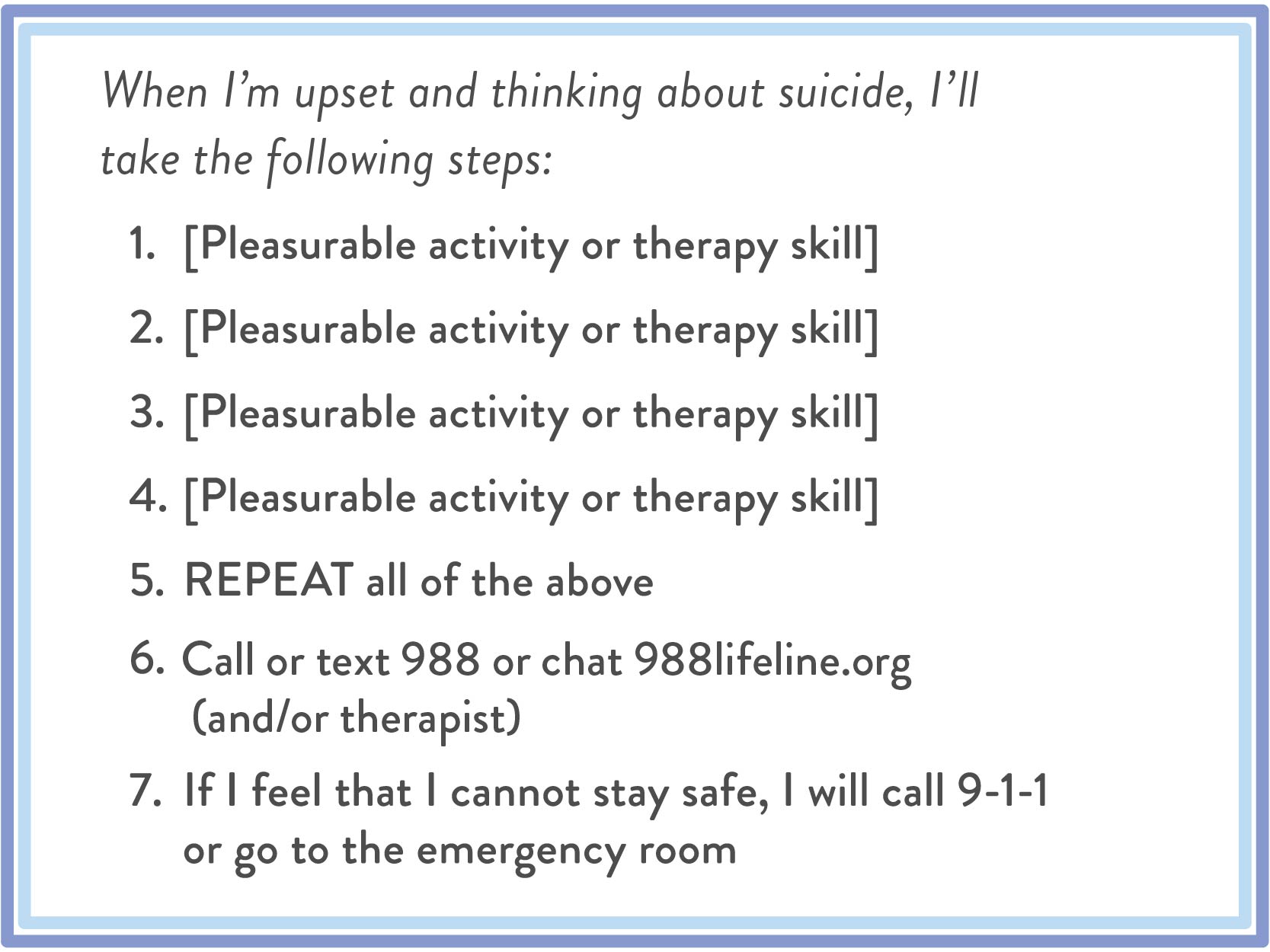 An example of a suicide prevention list that can be customized for the patient.
An example of a suicide prevention list that can be customized for the patient.A: Do not be afraid to say the words. If you are going to ask them if they are having thoughts of killing themselves, you have to ask it. If you don’t ask straightforwardly, you’re not going to know the answer to that question. Just saying it straight out is not going to change the conversation in any way that is going to make it worse.
Q: What’s your sense of how many health care professionals working with patients who have diabetes are screening for depression and suicide risk?
A: I would say there are definitely more clinics screening now than there were 10 years ago. Every practice should be doing this. We’re doing a disservice to our patients if we’re not asking about depression and suicide.
Q: What research is being conducted on the topic of suicide risk in patients with diabetes?
A: Looking specifically at suicide and diabetes, it’s a very under-researched, underfunded area. Some of the initial research is to figure out what the risk is and what do we do, from a clinical standpoint, for someone who’s at risk.
Research also needs to investigate differences in suicide risk among diabetes patients. Are there differences in terms of race, ethnicity, and socioeconomic status? Are there health disparities in terms of how we are screening, evaluating, and managing patients?
One thing we would really like to assess is prevention. Is there a way to identify somebody who is at risk for suicidal ideation and take preventative measures so they don’t get to that point?
How does your practice incorporate depression and suicide screening and assessment? Let us know in the comment section below.
Comments