

Pancreatic Islet Transplantation
On this page:
- What are islets?
- What is pancreatic islet transplantation and how can it treat type 1 diabetes?
- Who are candidates for islet transplantation?
- How do doctors perform islet transplantation?
- What are the benefits of islet transplantation?
- How successful is islet transplantation?
- What are the risks of islet transplantation?
- How common is islet transplantation?
- Why isn’t islet transplantation used more often to treat type 1 diabetes?
- Is islet transplantation used to treat any other conditions?
What are islets?
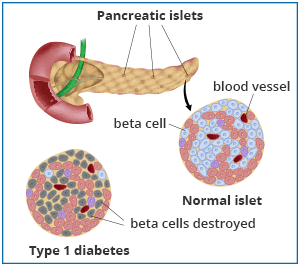
Pancreatic islets, also called islets of Langerhans, are groups of cells in your pancreas. The pancreas is an organ that makes hormones to help your body break down and use food. Islets contain several types of cells, including beta cells that make the hormone insulin. Insulin helps your body use glucose for energy and helps control your blood glucose levels, also called blood sugar.
What is pancreatic islet transplantation and how can it treat type 1 diabetes?
In people with type 1 diabetes, the body’s immune system attacks and destroys the beta cells. People with type 1 diabetes must take insulin because their bodies no longer make this hormone.
In the type of islet transplantation used to treat type 1 diabetes, also called islet allo-transplantation, doctors take islets with healthy beta cells from the pancreas of a deceased organ donor. Doctors then inject the healthy islet cells taken from the donor into a vein that carries blood to the liver of a person with type 1 diabetes. A person receiving a transplant is called a recipient. These islets begin to make and release insulin in the recipient’s body. More than one injection of transplanted islet cells is often needed to stop using insulin.
For many years, islet transplantation was considered experimental and was only performed in clinical trials. However, in 2023, the U.S. Food and Drug Administration (FDA) approved the first cell therapy made from islets of deceased donors for use in islet transplantation. This cell therapy is approved for adults with type 1 diabetes who have a hard time managing their blood glucose levels and continue to have repeated severely low blood glucose, also called severe hypoglycemia, despite intensive diabetes management and education.
Islet transplantation may help people with type 1 diabetes
- improve their blood glucose levels
- lower or remove the need for insulin injections
- better recognize symptoms of low blood glucose, also called hypoglycemia
- prevent severe hypoglycemia, which is when a person’s blood glucose level becomes so low that he or she needs help from another person to treat the hypoglycemia
A whole pancreas transplant is another procedure that can give a person with type 1 diabetes healthy beta cells. However, a pancreas transplant is a major surgery that carries a greater risk of complications than an islet transplant.
Who are candidates for islet transplantation?
Not all people with type 1 diabetes are good candidates for islet transplantation. Certain people with type 1 diabetes who have blood glucose levels that are difficult to manage, experience severe hypoglycemia, and have hypoglycemia unawareness—a dangerous condition in which a person can’t feel or recognize the symptoms of hypoglycemia—may be candidates.
Doctors consider people for islet transplantation if the possible benefits, such as being better able to reach blood glucose targets without problems such as hypoglycemia, outweigh the risks, such as the possible side effects of immunosuppressants. Immunosuppressants are medicines that recipients must take to prevent their immune system from attacking and destroying the transplanted islets.
People who have type 1 diabetes and have had, or are planning to have, a kidney transplant to treat kidney failure may be candidates for islet transplantation. Islet transplantation may be performed at the same time as or after a kidney transplant. Kidney transplant recipients will already be taking immunosuppressants to prevent rejection of the transplanted kidney. Therefore, the islet transplant does not add much more risk.
How do doctors perform islet transplantation?
Special enzymes are used to remove islets from the pancreas of a deceased donor. The islets are purified and counted in a lab. On average, about 400,000 islets are transplanted in each procedure.1
The transplant recipient will most often receive a local anesthetic and a sedative—medicine to help you relax—for the procedure. In some cases, the recipient may receive general anesthesia.
The islet transplant infusion procedure involves inserting a thin, flexible tube called a catheter through a small cut in the recipient’s upper abdomen. A radiologist uses x-rays and ultrasound to guide the catheter into the portal vein of the liver. The islets are slowly infused through the catheter and into the liver by gravity. Alternatively, a minimally invasive open procedure can be used to directly visualize a vein near the liver to insert the catheter.
Over the next 2 weeks, new blood vessels form and connect the islets with the blood vessels of the recipient.2 The beta cells in the islets begin to make and release insulin into the bloodstream immediately after transplant.
What are the benefits of islet transplantation?
Recipients may see the following benefits
- improved blood glucose levels
- less need or no need for insulin injections to manage diabetes
- fewer or no episodes of severe hypoglycemia
- improved awareness of hypoglycemia, which helps prevent episodes of severe hypoglycemia
Research also suggests that islet transplantation may prevent or slow the development of diabetes complications such as heart disease, kidney disease, and nerve or eye damage.3

How successful is islet transplantation?
A Phase 3 clinical trial conducted by the National Institutes of Health (NIH)-sponsored Clinical Islet Transplantation Consortium looked at outcomes associated with islet transplantation. Phase 3 trials test new treatments in large groups of people to confirm that treatments are effective and monitor side effects. Participants in this NIH-sponsored study included people with type 1 diabetes with problems managing their blood glucose levels, such as severe hypoglycemia and hypoglycemia unawareness.
The study found that, 1 year after islet transplantation, nearly 9 out of 10 transplant recipients had an A1C level below 7 percent and did not have episodes of severe hypoglycemia. The A1C goal for many people with diabetes is below 7 percent. About half of the recipients did not need to take any insulin. Two years after islet transplantation, about 7 out of 10 recipients had an A1C level of less than 7 percent and did not have episodes of severe hypoglycemia, and about 4 out of 10 did not need insulin.4
Ongoing research from this study also found that islet transplant recipients experienced significant improvements in their diabetes-related quality of life and reported better overall health status after the transplant. Even transplant recipients who still needed to take insulin to manage their diabetes experienced these improvements.5
What are the risks of islet transplantation?
Risks of islet transplantation include
- bleeding, blood clots, and pain after the procedure
- the chance that the transplanted islets may not work well or may stop working
- side effects of anti-rejection medicines, also called immunosuppressants, which are described below
- development of antibodies against the donor cells that may make it more difficult to find an appropriate organ donor if another transplant is needed in the future
Immunosuppressants
After an islet transplant, recipients will take medicines, called immunosuppressants, for as long as the transplanted islets are working. These medicines help prevent the body from rejecting the transplanted islets. Rejection occurs when the body’s immune system sees the islets as “foreign” and tries to destroy them. If the recipient stops taking immunosuppressants, the recipient’s body will reject the transplanted islets, and the islets will stop working.
Immunosuppressants can have many serious side effects. Possible side effects include
- a higher chance of getting infections
- a higher chance of getting cancer
- digestive side effects, such as vomiting, nausea, or diarrhea
- headaches, tremors, or confusion
- high blood pressure
- high blood glucose levels
- high levels of cholesterol and triglycerides in the blood
- kidney damage
How common is islet transplantation?
Islet transplantation is not a common treatment for type 1 diabetes. In the United States, islet transplantation was considered an experimental treatment for many years and was only performed in clinical trials. With the FDA approval of an islet cell therapy in 2023, islet transplantation is available outside of clinical trials to treat certain adults with type 1 diabetes.
The Collaborative Islet Transplantation Registry (CITR) has reported that, between 1999 and 2015, 1,086 people worldwide received islet transplants for type 1 diabetes.1 The CITR collects information on islet transplants performed at research centers in North America, Europe, Australia, and Asia. The National Institute of Diabetes and Digestive and Kidney Diseases established and supports the CITR. Breakthrough T1D, formerly known as JDRF or the Juvenile Diabetes Research Foundation, also helped establish CITR.
Why isn’t islet transplantation used more often to treat type 1 diabetes?
Islet transplantation is not often used to treat type 1 diabetes because recipients must take immunosuppressants, and donor islets are in short supply.
Islet transplant recipients must take immunosuppressants
Islet transplant recipients must take long-term immunosuppressants, and these medicines may cause serious side effects. Researchers are looking for ways to prevent islet rejection without long-term immunosuppressants. In one approach, called encapsulation, islets are coated with a material that protects them from being attacked by the recipient’s immune system.
Donor islets are in short supply
Only a small number of donor pancreases are available for islet transplantation each year. According to the Organ Procurement and Transplantation Network, 1,315 pancreases were recovered from deceased donors in 2017. Many donated pancreases are not suitable for islet isolation. Also, some donor islets may be damaged or destroyed during the transplant process.
Researchers are studying different ways to overcome the short supply of donor islets. For example, scientists are studying ways to transplant islets from pigs or create new human islets from stem cells.
Is islet transplantation used to treat any other conditions?
Doctors may perform a different type of islet transplantation, called islet auto-transplantation, in people who have their whole pancreas removed to treat severe and chronic pancreatitis. People with type 1 diabetes cannot receive islet auto-transplantation.
In islet auto-transplantation, doctors remove a patient’s pancreas, remove the islets from the pancreas, and transplant the islets into the patient’s liver. The goal is to give the body enough healthy islets that make insulin. Patients don’t need to take immunosuppressants after islet auto-transplantation because they receive islets from their own body.
Islet auto-transplantation is not considered experimental.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Rodolfo Alejandro, M.D., David Baidal, M.D., Ana Alvarez, APRN, Clinical Cell Transplant Program – Diabetes Research Institute, University of Miami Miller School of Medicine