

Ostomy Surgery of the Bowel
- Definition & Facts
- Types of Ostomy Surgery of the Bowel
- What to Expect Before & During Ostomy Surgery of the Bowel
- After Ostomy Surgery of the Bowel
- Complications of Ostomy Surgery of the Bowel
- Clinical Trials
Definition & Facts
In this section:
- What is ostomy surgery of the bowel?
- Does ostomy surgery of the bowel have other names?
- What is a stoma?
- Are there other names for a stoma?
- How common is ostomy surgery of the bowel?
- Why do people need ostomy surgery of the bowel?
What is ostomy surgery of the bowel?
Ostomy surgery of the bowel is an operation that changes the way intestinal contents—the waste products of digestion—leave your body when part or all of your bowel is diseased, injured, or missing. Creating an ostomy—or stoma—means bringing part of the bowel through the abdominal wall so that intestinal contents leave your body through the abdominal wall instead of passing through the anus.
The bowel is part of the digestive tract and is made up of the
- small intestine, which includes the duodenum, jejunum, and ileum. Most food digestion and nutrient absorption happen in your small intestine.
- large intestine, which includes the appendix, cecum, colon, and rectum. The large intestine takes in water from stool and changes it from a liquid to a solid form.
Does ostomy surgery of the bowel have other names?
Ostomy surgery of the bowel is also called bowel diversion or fecal diversion.
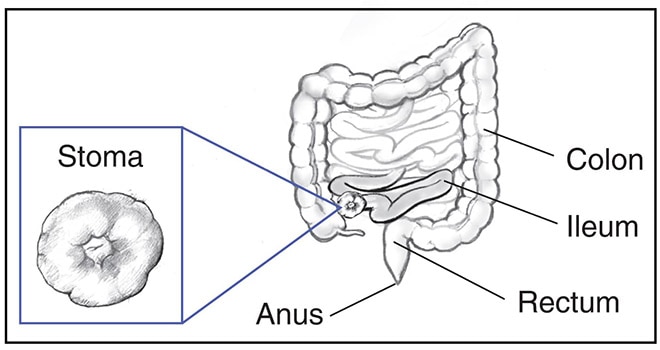
What is a stoma?
A stoma is a surgical connection between an internal organ and the skin on the outside of your body. During ostomy surgery of the bowel, surgeons create an opening through the skin and muscle of your abdomen and bring the large intestine or small intestine through this hole. The surgeon then connects the intestine to the skin on the outside. A stoma may be about 3/4 inch to about 2 inches wide.1,2
After ostomy surgery, intestinal contents will leave your body through the stoma. A stoma has no muscle, so it cannot control the timing or flow of intestinal contents. In most cases, you wear a removable pouch, called an ostomy pouch or ostomy appliance, that is attached to the skin around your stoma to collect the intestinal contents.
Your stoma may be temporary or permanent, depending on the reason you need ostomy surgery.

Are there other names for a stoma?
Health care professionals may use the name of the surgery to refer to the stoma created during the surgery. For example,
- a stoma created during any type of ostomy surgery may be called an ostomy
- a stoma created from the small intestine may be called an ileostomy
- a stoma created from the large intestine may be called a colostomy
How common is ostomy surgery of the bowel?
In the United States, about 100,000 people have ostomy surgery of the bowel each year.3
Why do people need ostomy surgery of the bowel?
Doctors may recommend ostomy surgery to help treat many different diseases and conditions, including
- birth defects that affect the anus or large intestine
- colorectal cancer and familial adenomatous polyposis, a condition that can lead to colorectal cancer
- diverticular disease
- inflammatory bowel disease, including Crohn’s disease and ulcerative colitis
- injury to the bowel
- intestinal obstruction
Doctors may also recommend a temporary stoma if all or part of your large intestine needs time to rest after surgery. Intestinal contents will leave the body through the stoma before reaching the part of the intestine that needs to recover.
References
Types of Ostomy Surgery of the Bowel
What are the types of ostomy surgery of the bowel?
The most common types of ostomy surgery of the bowel include ileostomy, colostomy, and continent ileostomy. Ileoanal pouch surgery is another type of bowel surgery that usually requires a temporary ileostomy. The type of surgery your doctor recommends may depend on why you need surgery and other factors.
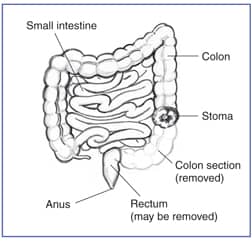
Ileostomy and colostomy
Ileostomy and colostomy are procedures that connect the bowel to the skin on the outside of your abdomen.
- In ileostomy, surgeons bring the ileum—the end part of your small intestine—through the abdominal wall and create a stoma. The entire large intestine is bypassed or removed.
- In colostomy, surgeons bring the colon—part of your large intestine—through the abdominal wall and create a stoma. The part of your large intestine below the stoma is bypassed or removed.
Surgeons most often construct the stoma so it sticks out above the surface of the skin, which may lower the risk of stoma problems after surgery.
Your stoma may be temporary if all or part of your large intestine needs time to rest or heal after injury, infection, or surgery. When the large intestine recovers, you’ll have a second surgery to close the ostomy. After this procedure, intestinal contents will move through the intestines, and stool will pass through the anus again.
Your stoma will be permanent if your large intestine and anus are removed or cannot heal or work properly again.
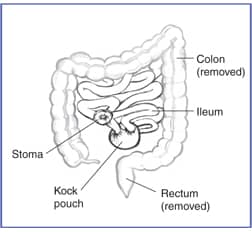
Continent ileostomy
During continent ileostomy, surgeons create an internal pouch—sometimes called a Kock pouch—from the ileum and make a valve inside the pouch. Surgeons bring the end of the ileum through the abdominal wall to create a stoma next to the pouch. After surgery, the valve will prevent intestinal contents from flowing out of the stoma. You’ll drain the pouch a few times each day by inserting a tube, called a catheter, through the stoma.
Continent ileostomy is less common than other types of ostomy surgery. Your doctor may refer you to a specialized medical center where surgeons perform this type of surgery.
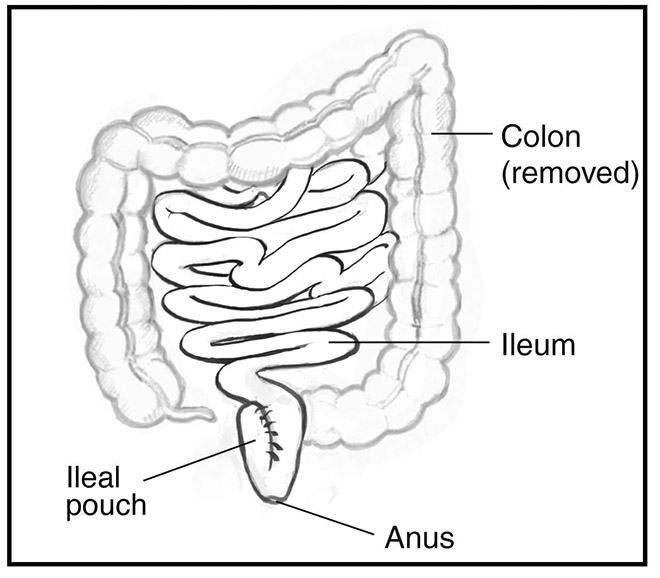
Ileoanal pouch surgery
Ileoanal pouch surgery—also called ileal pouch anal anastomosis, or IPAA—may be performed in one, two, or three operations. Surgeons most often complete this procedure in two operations.
- During the first operation, surgeons remove the large intestine, create a pouch from part of the ileum, and attach the pouch to the anus. Surgeons also perform an ileostomy above the pouch, creating a temporary stoma.
- If the pouch heals properly, during the second operation surgeons close the temporary ileostomy.
After ileoanal pouch surgery, stool will leave your body through the anus during bowel movements. Most people are continent, meaning they are able to control the timing of bowel movements, but the bowel movements are much looser and more frequent than with a healthy colon in place.
What to Expect Before & During Ostomy Surgery of the Bowel
How do I prepare for ostomy surgery of the bowel?
Your surgeon and an ostomy nurse may help you prepare for ostomy surgery of the bowel. Ostomy nurses—wound, ostomy, and continence nurses or enterostomal therapy nurses—are nurses who specialize in ostomy care.
An ostomy nurse can help you prepare for ostomy surgery by providing information about topics such as
- the surgical procedure you will have
- how ostomy pouches work
- how to adjust to life with a stoma
Health care professionals will examine you while you are in different positions—such as standing, sitting, or lying down—to help decide where the stoma should be placed. Stomas are usually placed in the lower part of the abdomen, just below the beltline. However, people who have obesity typically need the stoma to be placed in the upper abdomen.
Your surgeon and ostomy nurse will help choose a location for your stoma that
- you can easily see and reach
- will be less likely to get in the way of your activities or clothing
- will lower the chance of complications after surgery

How do surgeons perform ostomy surgery of the bowel?
How your surgeon performs ostomy surgery will depend on the type of surgery you are having. You will receive general anesthesia for ostomy surgery.
Surgeons may perform laparoscopic, robotic, or open ostomy surgery. During laparoscopic and robotic surgery, surgeons make a small cut in your abdomen and insert a laparoscope—a thin tube with a tiny video camera and light attached—to view the inside of your abdomen. Surgeons will then make additional small cuts and insert tools to remove or repair organs and tissues. In open surgery, surgeons make a larger cut to open your abdomen.
Depending on the reason you need surgery, surgeons may also remove or repair part of the digestive tract during the operation.
After Ostomy Surgery of the Bowel
In this section:
- What should I expect after ostomy surgery of the bowel?
- How does ostomy surgery of the bowel change my digestive tract?
- How will I manage waste and gas?
- Will my diet need to change?
- When can I go back to my usual activities?
- How can I cope with practical, social, and emotional issues after ostomy surgery?
What should I expect after ostomy surgery of the bowel?
Most people are able to lead full and active lives and return to most of the activities they enjoyed before ostomy surgery. As you adjust to life after your ostomy surgery, your ostomy nurse will provide education, support, and medical advice.
Your ostomy nurse may cover topics that include
- understanding changes to your digestive tract
- managing waste and gas
- eating a healthy diet and drinking enough liquids
- recovering from surgery and returning to your usual activities
- coping with practical, social, and emotional issues
- watching for and preventing complications
How does ostomy surgery of the bowel change my digestive tract?
During ostomy surgery, surgeons remove or bypass
- all or part of the large intestine. The large intestine usually takes in water from stool and changes it from a liquid to a solid form. The large intestine includes the colon and rectum.
- part of the small intestine, in some cases. The small intestine usually absorbs nutrients from the foods you eat.
Depending on how much of your large or small intestine were removed or bypassed, you may experience some changes or problems with your digestive tract and how it works.
- Your stool may be less solid and formed.
- Your digestive tract may absorb less water and nutrients.
- You may have digestive symptoms such as gas, diarrhea, or constipation. These symptoms may improve over time as the digestive tract heals and you add more foods to your diet.
- If your rectum was removed, you may experience phantom rectum. Phantom rectum is the feeling that you need to have a bowel movement, even though your rectum is no longer there.
- If the lower part of your digestive tract and anus were bypassed but not removed, the bypassed digestive tract may still produce mucus, which may leak or pass from the anus.
Health care professionals can recommend strategies or treatments to help you manage changes in your digestive tract after surgery.
How will I manage waste and gas?
Surgery changes the way the contents of the digestive tract leave your body. Your ostomy nurse will teach you how to manage waste and gas, based on the type of ostomy surgery you had.
Ileostomy or colostomy
If you had an ileostomy or colostomy, your ostomy nurse will help you choose an ostomy pouch—also called a pouching system or appliance. An ostomy pouch is a removable pouch you wear outside your body, attached to the skin around your stoma. The ostomy pouch will collect intestinal contents and gas that pass from your stoma.
Different types of pouching systems are available, and your ostomy nurse can help you choose the system that’s right for you. Pouching systems include a skin barrier—also called a wafer or flange—that sticks to the skin around the stoma and protects the skin from intestinal contents, which can cause irritation. The systems also include a disposable, odor-proof pouch that collects intestinal contents. The skin barrier and pouch may be one piece or two separate pieces. The ostomy pouch is emptied one or more times per day, while the wafer is changed about every 3 days.4
Your ostomy nurse can provide information about
- how to use your pouching system, including how often to empty and change the pouch or pouching system
- how to clean and care for your stoma and the skin around it
- how to check for signs of problems or complications when you change your ostomy pouch
Continent ileostomy
If you had a continent ileostomy, you won’t need to wear an ostomy pouch. Your ostomy nurse will teach you how to insert a tube, called a catheter, into the stoma to drain the internal pouch.
Ileoanal pouch surgery
After ileoanal pouch surgery is complete, the temporary stoma is closed. Stool and gas will leave your body through your anus, as they did before surgery. At first, you will have more frequent bowel movements, up to 15 per day.5 You may have mild bowel control problems and may need to wake up from sleep to pass stool. The newly formed pouch will take several months to stretch and adjust to its new function. Over time, people typically have fewer bowel movements and bowel control problems. On average, people who had ileoanal pouch surgery have about seven bowel movements per day, including one at night.6
Will my diet need to change?
After ostomy surgery, many people are eventually able to go back to their regular diet and eat and drink what they like. In some cases, health care professionals may recommend diet changes based on a person’s medical conditions or the type of ostomy surgery he or she had.
Talk with your doctor and ostomy nurse about healthy eating. Your doctor may refer you to a registered dietitian to help you create a healthy eating plan.
For the first several weeks after surgery, health care professionals may recommend
- eating a healthy diet that provides the nutrients you need while you recover from surgery
- drinking enough liquids to prevent dehydration
- avoiding high-fiber foods such as raw fruits and vegetables, seeds, nuts, and corn
- avoiding spicy or high-fat foods
Health care professionals may recommend adding new foods to your diet gradually, after you recover from surgery. Just as before ostomy surgery, certain foods are more likely to cause digestive symptoms such as constipation, diarrhea, gas, or stool odor. Keeping a food journal can help you track the foods you eat and how they affect you.
Talk with your doctor, ostomy nurse, or registered dietitian about any digestive problems you have. Health care professionals may recommend diet changes, medicines, or other treatments to manage these problems.

When can I go back to my usual activities?
For some time after surgery, your doctor may recommend you rest and avoid certain activities, such as driving or heavy lifting. Follow your doctor’s instructions about when you can go back to your usual work and leisure activities.
Once you recover from surgery, you should be able to return to most of the activities you enjoyed before surgery, including swimming and other water sports. Your ostomy nurse can advise you about managing your ostomy pouch, if you have one, during physical activity.
Certain types of activities, such as contact sports and heavy lifting, could risk injury to your stoma. Your doctor or nurse may recommend avoiding these activities or taking steps to protect your stoma and prevent injury.
How can I cope with practical, social, and emotional issues after ostomy surgery?
You may face practical, social, and emotional issues as you adjust to life after ostomy surgery. Your ostomy nurse and other health care professionals can answer your questions and provide information, advice, and support related to a variety of issues, including
- feelings and emotions, including body image
- intimacy and sexual activity
- maintaining personal relationships, including talking about your ostomy surgery with family, friends, and others
- social life and travel
Support from family members, partners, and health care professionals can help you adjust to life after ostomy surgery. Your ostomy nurse can refer you to community or online resources and support groups that may be helpful as you adjust.
References
Complications of Ostomy Surgery of the Bowel
What complications may occur after ostomy surgery of the bowel?
Talk with your doctor, surgeon, or ostomy nurse about possible complications that may occur after your surgery. Like any major surgery, ostomy surgery may lead to complications, such as bleeding and infection. Some risks depend on the type of ostomy surgery you have and the reasons you need surgery.
After ostomy surgery, talk with your ostomy nurse or doctor if you notice any unusual symptoms or problems. They may recommend at-home treatments for minor problems or complications. Doctors may recommend medicines, surgery, or other medical treatments for more serious complications.
Ileostomy or colostomy
Complications of ileostomy and colostomy may include stoma or skin complications, dehydration, problems absorbing nutrients, and intestinal obstruction.
Stoma complications
Complications that are more common within the first 30 days after surgery may include7,8
- bleeding from the stoma
- lack of blood supply to the stoma and death of stoma tissue
- retraction, or when the stoma sinks below the level of the skin
- separation of the stoma from the skin around it
Stoma complications that are more common 30 days or later after surgery may include7,8
- hernia, or abdominal contents bulging through a weak area in the abdominal wall near the stoma. In rare cases, part of the intestine may become stuck in the hernia, which can lead to a blockage in the intestine or cause the intestine to lose its blood supply.
- prolapse, or when part of the intestine pushes itself through the stoma. Rarely, the prolapsed intestine may become stuck in the stoma and lose its blood supply.
- retraction.
- stricture, or narrowing of the stoma, which makes it difficult for intestinal contents to pass.
Skin complications
Complications involving the skin around the stoma are common. Skin complications may include
- irritation when intestinal contents that leak from the stoma touch the skin, which can happen if your ostomy pouch doesn’t fit properly
- irritation or injury related to applying or changing your ostomy pouch
- infection with bacteria or fungi
Other complications
After ileostomy or colostomy, other complications may include
- dehydration, which is more common if all of your large intestine was removed or bypassed
- problems absorbing nutrients, which may occur if part of your small intestine was removed or bypassed
- intestinal obstruction, a partial or complete blockage of food, fluids, air, or stool moving through your intestines
Continent ileostomy
Complications of continent ileostomy may include
- problems with the pouch, such as pouchitis
- problems with the stoma, such as stricture or hernia
- problems with the valve, which may make it hard to drain the pouch or cause incontinence
- small intestinal obstruction
Ileoanal pouch surgery
Complications of ileoanal pouch surgery that are more common within the first 30 days after surgery may include9,10
- blood clots in the portal vein
- pelvic sepsis, or infection in the lower abdomen around the ileoanal pouch, which may cause abscesses or fistulas to form
- small intestinal obstruction
Complications that are more common 30 days or later after surgery may include9,10
- pouchitis, which is inflammation of the ileoanal pouch
- cuffitis, which is inflammation of the area where surgeons attached the pouch to the anus
- small intestinal obstruction
- stricture, or narrowing of the area where the ileoanal pouch is connected to the anus
After ileoanal pouch surgery, more frequent bowel movements may cause the skin around your anus to become irritated. Your ostomy nurse will teach you how to prevent and treat irritated skin.

Seek medical help right away
Contact your doctor or ostomy nurse if you notice any unusual signs and symptoms any time after ostomy surgery.
Talk with your doctor and ostomy nurse about symptoms that could be signs of a serious complication and when you should contact a health care professional or seek emergency medical care.
Seek medical help right away if you have symptoms that could be related to a serious complication. Examples include1,2,5
- problems with your stoma, such as changes in a stoma’s size, shape, color, or odor; bleeding from inside or around the stoma that is heavy or doesn’t stop; or an injury or deep cut to the stoma
- cramping in the abdomen that lasts for more than 2 or 3 hours
- nausea and vomiting that is severe or does not stop
- passing no gas or stool from a stoma for more than 4 to 6 hours, along with cramping and nausea
- severe diarrhea or watery output from a stoma, which could lead to dehydration
References
Clinical Trials
The NIDDK conducts and supports clinical trials in many diseases and conditions, including digestive diseases. The trials look to find new ways to prevent, detect, or treat disease and improve quality of life.
What are clinical trials for ostomy surgery?
Clinical trials—and other types of clinical studies—are part of medical research and involve people like you. When you volunteer to take part in a clinical study, you help doctors and researchers learn more about disease and improve health care for people in the future.
Researchers are studying many aspects of ostomy surgery of the bowel, including helping people adjust to living with a stoma after ostomy surgery. Find out if clinical studies are right for you.
Watch a video of NIDDK Director Dr. Griffin P. Rodgers explaining the importance of participating in clinical trials.
What clinical studies for ostomy surgery are looking for participants?
You can view a filtered list of clinical studies on ostomy surgery that are federally funded, open, and recruiting at ClinicalTrials.gov. You can expand or narrow the list to include clinical studies from industry, universities, and individuals; however, the National Institutes of Health does not review these studies and cannot ensure they are safe. Always talk with your health care provider before you participate in a clinical study.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Samantha Hendren, M.D., M.P.H., University of Michigan