

Adrenal Insufficiency & Addison’s Disease
Return to Overview PageDefinition & Facts
In this section:
- What is adrenal insufficiency?
- What do adrenal hormones do?
- How common is adrenal insufficiency?
- Who is more likely to develop adrenal insufficiency?
- What are the complications of adrenal insufficiency?
What is adrenal insufficiency?
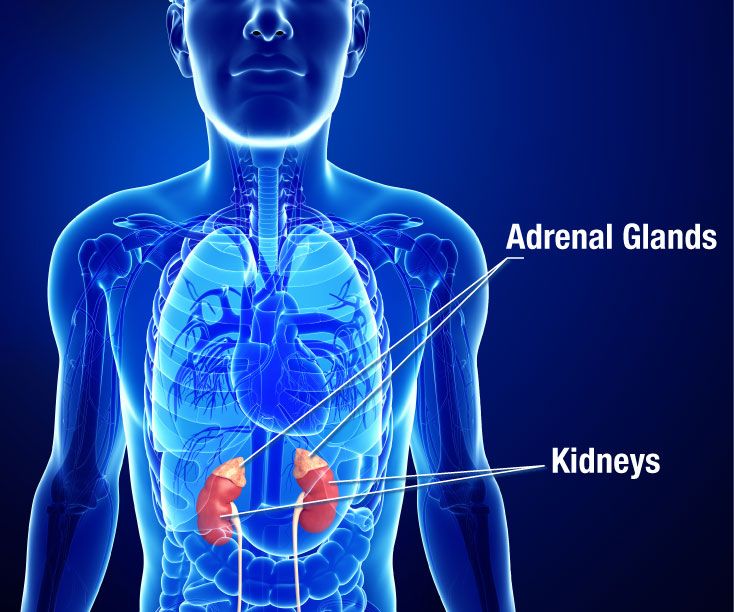
Adrenal insufficiency is a disorder that occurs when the adrenal glands don’t make enough of certain hormones. The adrenal glands are located just above the kidneys. Adrenal insufficiency can be primary, secondary, or tertiary. Primary adrenal insufficiency is often called Addison’s disease.
Adrenal insufficiency can affect your body’s ability to respond to stress and maintain other essential life functions. With treatment, most people with adrenal insufficiency can have a normal, active life.
Addison's disease
Addison’s disease occurs when the adrenal glands are damaged and can’t make enough of the hormone cortisol and sometimes the hormone aldosterone.
Secondary adrenal insufficiency
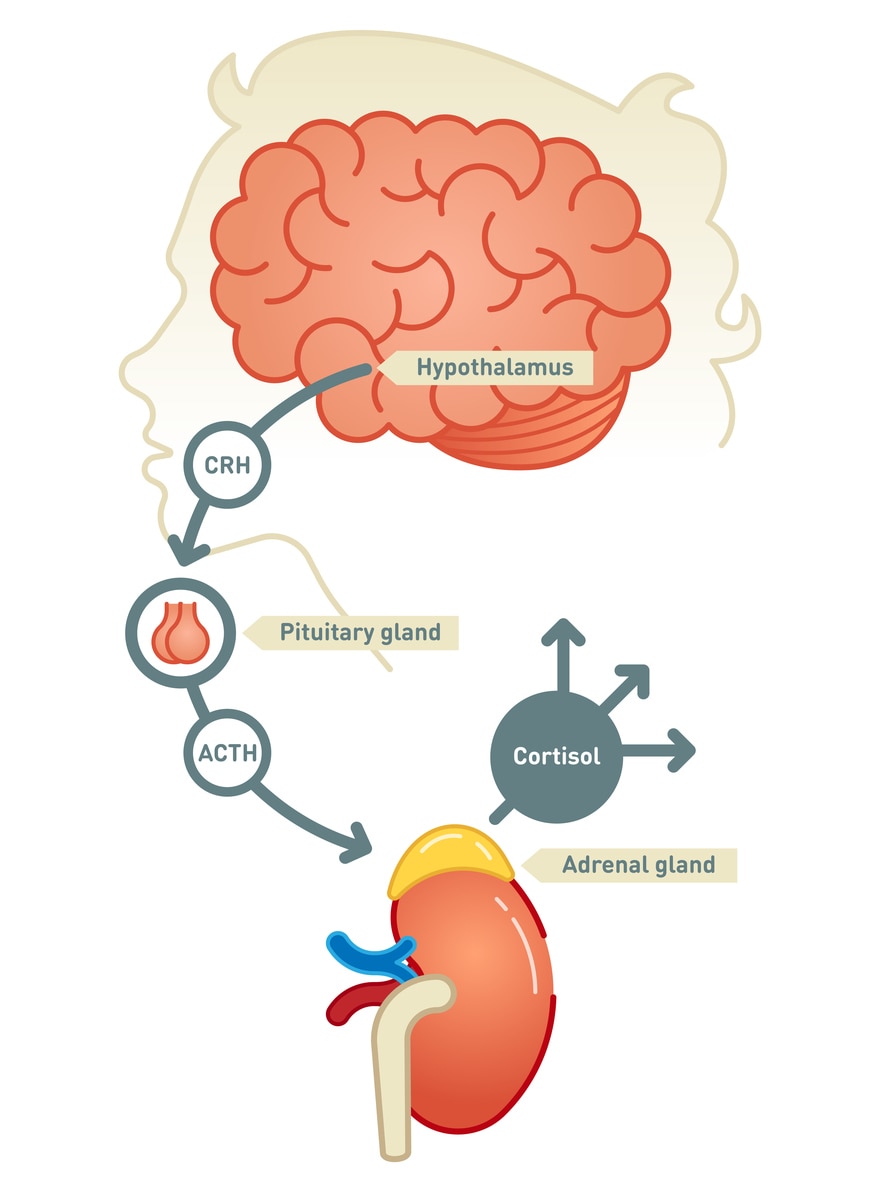
Secondary adrenal insufficiency starts in the pituitary—a pea-sized gland at the base of the brain. The pituitary makes adrenocorticotropin (ACTH), a hormone that tells the adrenal glands to make cortisol. If the pituitary doesn’t make enough ACTH, the adrenal glands don’t make enough cortisol. Over time, the adrenal glands can shrink and stop working.
Tertiary adrenal insufficiency
Tertiary adrenal insufficiency starts in the hypothalamus, a small area of the brain near the pituitary. The hypothalamus makes corticotropin-releasing hormone (CRH), a hormone that tells the pituitary to make ACTH. When the hypothalamus doesn’t make enough CRH, the pituitary gland doesn’t make enough ACTH. In turn, the adrenal glands don’t make enough cortisol.
What do adrenal hormones do?
The adrenal glands make two main types of hormones: cortisol and aldosterone.
Cortisol
Cortisol is sometimes called the “stress hormone” because it helps your body respond to stress. Cortisol also helps
- control blood pressure
- control blood glucose, also called blood sugar
- reduce inflammation
- control metabolism
Cortisol belongs to a class of hormones called glucocorticoids.
Aldosterone
Aldosterone helps maintain the balance of the minerals sodium and potassium in your blood. Sodium and potassium work together to control the salt and water balance in your body and help keep blood pressure stable. Both help maintain normal nerve and muscle function. Potassium also helps your heartbeat stay regular.
Aldosterone belongs to a class of hormones called mineralocorticoids.
How common is adrenal insufficiency?
Addison’s disease is rare. In developed countries, it affects about 100 to 140 of every million people.1
Secondary adrenal insufficiency is more common, affecting 150 to 280 people per million.2,3 Secondary and tertiary adrenal insufficiency are often grouped together, so no numbers for tertiary adrenal insufficiency by itself are available.
Who is more likely to develop adrenal insufficiency?
Women are more likely than men to develop Addison’s disease.3 This condition occurs most often in people between the ages of 30 and 50,2 although it can occur at any age, even in children.
Secondary adrenal insufficiency occurs in people with certain conditions that affect the pituitary.
People who take glucocorticoid medicines, such as prednisone, for a long time and then stop are most likely to develop tertiary adrenal insufficiency. These medicines are used to treat medical conditions such as asthma, rheumatoid arthritis, lupus, cancer, and inflammation, among others.
What are the complications of adrenal insufficiency?
The most serious complication of adrenal insufficiency is called adrenal crisis. If not treated right away, adrenal crisis can cause death. Your body needs much more cortisol than usual during times of physical stress such as illness, serious injury, or surgery. The severe lack of cortisol at these times can cause life-threatening low blood pressure, low blood glucose, low blood sodium, and high blood potassium.
Sometimes the lack of aldosterone in Addison’s disease can cause hyponatremia. This condition occurs when you don’t have enough sodium in your blood. Hyponatremia can cause confusion, fatigue, and muscle twitches and seizures. The lack of aldosterone can also cause hyperkalemia, or too much potassium. Mild hyperkalemia may not cause problems, but severe hyperkalemia can cause life-threatening changes in your heart rhythm.
References
Symptoms & Causes
What are the symptoms of adrenal insufficiency?
The most common symptoms of adrenal insufficiency are
- chronic, or long-lasting, fatigue
- muscle weakness
- loss of appetite
- weight loss
- abdominal pain

Other symptoms of adrenal insufficiency can include
- nausea
- vomiting
- diarrhea
- low blood pressure that drops further when you stand up, causing dizziness or fainting
- irritability and depression
- joint pain
- craving salty foods
- hypoglycemia, or low blood glucose
- irregular or no menstrual periods
- loss of interest in sex
People with Addison’s disease may also have darkening of their skin. This darkening is most visible on scars; skin folds; pressure points such as the elbows, knees, knuckles, and toes; lips; and mucous membranes such as the lining of the cheek.
Because symptoms of adrenal insufficiency come on slowly over time, they may be overlooked or confused with other illnesses. Sometimes symptoms appear for the first time during adrenal crisis. If you always feel tired, weak, or are losing weight, ask your health care professional if you might have adrenal insufficiency. Early treatment can help avoid an adrenal crisis.
What causes adrenal insufficiency?
Different types of adrenal insufficiency have different causes. The most common cause of adrenal insufficiency overall is suddenly stopping corticosteroids after taking them for a long time.
Addison’s disease
Damage to the adrenal glands in Addison’s disease is usually caused by autoimmune disease—when your immune system attacks your body’s own cells and organs. In developed countries, autoimmune disease causes 8 or 9 of every 10 cases of Addison’s disease.4
Certain infections can also cause Addison’s disease. Tuberculosis (TB) can damage the adrenal glands and used to be the most common cause of Addison’s disease. As treatment improved over the years, TB became a much less common cause. People with HIV/AIDS, whose weakened immune systems can’t fight off infections that could cause Addison’s disease, are also at risk.
Less common causes of Addison’s disease are
- cancer cells in the adrenal glands
- surgical removal of the adrenal glands to treat other conditions
- bleeding into the adrenal glands
- genetic disorders that affect the way the adrenal glands develop or function
- certain medicines, such as antifungal medicines or etomidate, a type of general anesthesia
Secondary adrenal insufficiency
Anything that affects the pituitary’s ability to make ACTH can cause secondary adrenal insufficiency. The pituitary makes many different hormones, so ACTH may not be the only hormone that’s lacking.
Causes of secondary adrenal insufficiency include
- autoimmune disease
- pituitary tumors or infection
- bleeding in the pituitary
- genetic diseases that affect the way the pituitary gland develops or functions
- surgical removal of the pituitary to treat other conditions
- traumatic brain injury
Tertiary adrenal insufficiency
The most common cause of tertiary adrenal insufficiency is suddenly stopping corticosteroids after taking them for a long time. Prescription doses of corticosteroids can cause higher levels of cortisol in your blood than your body normally makes. High levels in your blood for a long time cause the hypothalamus to make less CRH. Less CRH means less ACTH, which in turn causes the adrenal glands to stop making cortisol.
Once you stop taking corticosteriods, your adrenal glands may be slow to start working again. To give them time to start making cortisol again, your doctor will gradually reduce your dose over a period of weeks or even months. Even so, your adrenal glands might not begin to work normally for many months. Your doctor should watch you carefully for symptoms of adrenal insufficiency.
Tertiary adrenal insufficiency can also occur after Cushing’s syndrome is cured. Cushing’s syndrome is a hormonal disorder caused by high levels of cortisol in the blood for a long time. Sometimes Cushing’s syndrome is caused by tumors, usually noncancerous, in the pituitary or adrenal glands that make too much ACTH or cortisol. Once the tumors are surgically removed, the source of excess ACTH or cortisol is suddenly gone. Your adrenal glands may be slow to start working again.
Reference
Diagnosis
How do doctors diagnose adrenal insufficiency?
Your doctor will review your symptoms and run tests to confirm that your cortisol levels are low.
Review of symptoms
In its early stages, adrenal insufficiency can be hard to diagnose since symptoms come on slowly. Your health care professional may suspect it after reviewing your medical history and symptoms. The next step is blood testing to see if your cortisol levels are too low and to help find the cause.
Blood tests
ACTH stimulation test
The ACTH stimulation test is the test used most often to diagnose adrenal insufficiency. In this test, a health care professional will give you an intravenous (IV) injection of man-made ACTH, which is just like the ACTH your body makes. Your health care professional will take samples of your blood before and 30 minutes or 60 minutes after the injection. The cortisol levels in your blood samples are measured in a lab.

The normal response after an ACTH injection is a rise in blood cortisol levels. People with Addison’s disease and most people who have had secondary adrenal insufficiency for a long time have little or no increase in cortisol levels. The adrenal glands may be too damaged to respond to ACTH.
The ACTH test may not be accurate in people who have had secondary adrenal insufficiency for a shorter time because their adrenal glands have not yet shrunk and can still respond to ACTH.
Insulin tolerance test
If the results of the ACTH stimulation test aren’t clear or your doctor suspects a problem in the pituitary, you may have an insulin tolerance test (ITT). A health care professional will give you an IV injection of the hormone insulin, which lowers your levels of blood glucose. The dose is high enough to cause hypoglycemia, which occurs when your blood glucose level drops too low.
Hypoglycemia causes physical stress, which normally triggers the pituitary to make more ACTH. A health care professional will draw your blood at the beginning of the test and again every half hour during the next 2 hours. If your cortisol levels are low, your pituitary isn’t making enough ACTH, so your adrenal glands don’t make enough cortisol. The ITT is the most reliable test to diagnose secondary adrenal insufficiency.
Very low blood glucose levels can be dangerous, so a health care professional must be present at all times during this test to make sure blood glucose levels don’t drop too low. The ITT isn’t safe for people with heart disease, a history of seizures, and other serious illnesses.
CRH stimulation test
The CRH stimulation test is another option to help identify secondary insufficiency if the results of the ACTH test aren’t clear. This test can also tell secondary from tertiary adrenal insufficiency.
A health care professional will give you an IV injection of CRH and take samples of your blood before and 30, 60, 90, and 120 minutes after the injection to measure ACTH levels. If the pituitary is damaged, it won’t make ACTH in response to the CRH injection. This result shows secondary adrenal insufficiency. A slow rise in ACTH levels suggests tertiary adrenal insufficiency.
What tests do doctors use to find the cause of adrenal insufficiency?
Once doctors diagnosis and identify the type of adrenal insufficiency, they may use blood and imaging tests to find the exact cause.
Addison’s disease
Antibody blood tests
A blood test can find antibodies that are present in autoimmune Addison’s disease. Antibodies are proteins made by your immune system to protect your body from bacteria or viruses. In autoimmune Addison’s disease, the antibodies mistakenly attack the adrenal glands. Most, but not all, people with autoimmune Addison’s disease have these antibodies. If the test shows antibodies, you don’t need further testing.
Computed tomography (CT) scan
CT scans use a combination of x-rays and computer technology to create images of your organs and other internal structures. A CT scan of the abdomen can find changes in your adrenal glands. In autoimmune Addison’s disease, the glands are small or normal size and don’t have other visible abnormalities.

Enlarged adrenal glands or a buildup of calcium in the glands can occur when Addison’s disease is caused by infection, bleeding in the adrenal glands, or cancer cells in the glands. However, these changes don’t always occur in Addison’s disease caused by TB.
Tests for TB
Tests to find TB include a chest x-ray, a urine test to look for the bacteria that causes TB, and a TB skin test. In the skin test, a health care professional injects a tiny amount of inactive TB bacteria under the skin of your forearm. If you develop a hard, raised bump or swelling on your arm, you have the TB bacteria in your body, even if you don’t have active TB.
Secondary and tertiary adrenal insufficiency
Magnetic resonance imaging (MRI)
MRI machines use radio waves and magnets to create detailed pictures of your internal organs and soft tissues without using x-rays. An MRI can look for changes in your pituitary and hypothalamus, such as large, noncancerous pituitary tumors.
Treatment
How do doctors treat adrenal insufficiency?
Your doctor will prescribe hormone medicines to replace the hormones that your adrenal glands aren’t making. You’ll need higher doses during times of physical stress.
Hormone replacement
Cortisol is replaced with a corticosteroid, most often hydrocortisone, which you take two or three times a day by mouth. Less often, doctors prescribe prednisone or dexamethasone.
If your adrenal glands aren’t making aldosterone, you will take a medicine called fludrocortisone, which helps balance the amount of sodium and fluids in your body. People with secondary adrenal insufficiency usually make enough aldosterone, so they don’t need to take this medicine.
Your doctor will adjust the dose of each medicine to meet your body’s needs.
Treatment for adrenal crisis includes immediate IV injections of corticosteroids and large amounts of IV saline, a salt solution, with dextrose added. Dextrose is a type of sugar.
Treatment in special situations
Surgery
If you’re having any type of surgery that uses general anesthesia, you may have treatment with IV corticosteroids and saline. IV treatment begins before surgery and continues until you’re fully awake after surgery and can take medicine by mouth. Your doctor will adjust the “stress” dose as you recover until you’re back to your pre-surgery dose.

Illness
Talk with your doctor about how to adjust your dose of corticosteroids during an illness. You will need to increase your dose if you have a high fever. Once you recover, your doctor will adjust your dose back to your regular, pre-illness level. You will need immediate medical attention if you have a severe infection or diarrhea, or are vomiting and can’t keep your corticosteroid pills down. Without treatment, in an emergency room if necessary, these conditions can lead to an adrenal crisis.
Injury or other serious condition
If you have a severe injury, you may need a higher, “stress” dose of corticosteroids right after the injury and while you recover. The same is true if you have a serious health condition such as suddenly passing out or being in a coma. Often, you must get these stress doses intravenously. Once you recover, your doctor will adjust your dose back to regular, pre-injury level.
Pregnancy
If you become pregnant and have adrenal insufficiency, you’ll take the same dose of medicine as you did before pregnancy. However, if nausea and vomiting in early pregnancy make it hard to take medicine by mouth, your doctor may need to give you corticosteroid shots. During delivery, treatment is similar to that of people needing surgery. Following delivery, your doctor will slowly decrease your dose, and you’ll be back to your regular dose about 10 days after your baby is born.
Eating, Diet, & Nutrition
What should I eat if I have adrenal insufficiency?
Some people with Addison’s disease who have low aldosterone can benefit from a high-sodium diet. A health care professional or a dietitian can recommend the best sodium sources and how much sodium you should have each day.
High doses of corticosteroids are linked to a higher risk of osteoporosis—a condition in which the bones become less dense and more likely to fracture. If you take corticosteroids, you may need to protect your bone health by getting enough dietary calcium and vitamin D. A health care professional or a dietitian can tell you how much calcium you should have based on your age. You may also need to take calcium supplements.

Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions, including adrenal insufficiency.
What are clinical trials for adrenal insufficiency?
Clinical trials—and other types of clinical studies—are part of medical research and involve people like you. When you volunteer to take part in a clinical study, you help doctors and researchers learn more about disease and improve health care for people in the future.
Researchers are studying many aspects of adrenal insufficiency to
- Learn more about conditions that affect the endocrine glands
- Identify effective treatment regimens
Find out if clinical studies are right for you.
Watch a video of NIDDK Director Dr. Griffin P. Rodgers explaining the importance of participating in clinical trials.
What clinical trials for adrenal insufficiency are looking for participants?
You can view a filtered list of clinical studies on adrenal insufficiency that are open and recruiting at ClinicalTrials.gov. You can expand or narrow the list to include clinical studies from industry, universities, and individuals; however, the NIH does not review these studies and cannot ensure they are safe. Always talk with your health care provider before you participate in a clinical study.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Constantine Stratakis, M.D., D.Med. Sci., Eunice Kennedy Shriver National Institute of Child Health and Human Development, NIH