

Weight-loss (Metabolic & Bariatric) Surgery
- Definition & Facts
- Types of Weight-loss Surgery
- Weight-loss Surgery Benefits
- Weight-loss Surgery Side Effects
- Potential Candidates for Weight-loss Surgery
- Clinical Trials
Definition & Facts
In this section:
- What is weight-loss surgery?
- Who are good candidates for weight-loss surgery?
- Does weight-loss surgery always work?
- How much does weight-loss surgery cost?
What is weight-loss surgery?
Weight-loss surgery encompasses a group of operations that help you lose weight by making changes to your digestive system. It is also known as metabolic and bariatric surgery ("metabolic" means "related to how your body gets energy" and "bariatric" means "related to treatment for heavy weight").
Some types of weight-loss surgery make your stomach smaller, limiting how much you can eat and drink at one time, so you feel full sooner. Other types of weight-loss surgery change your small intestine—the part of your digestive system that absorbs energy and nutrients from foods and beverages. These types of surgery reduce the number of calories the body can absorb. Weight-loss surgery also can affect hormones or bacteria in the gastrointestinal tract in ways that may reduce appetite and hunger and improve how the body metabolizes fat and makes use of insulin.
Who are good candidates for weight-loss surgery?
You may be a good candidate for weight-loss surgery if you are an adult who has obesity and you have not been able to lose your excess weight, or you keep gaining back weight you have lost using other methods such as eating plans, exercise, or medications.
Body Mass Index (BMI) is a measure of obesity used to determine who are good candidates for weight-loss surgery. BMI measures body fat based on weight in relation to height. For people with a BMI of 35 or higher, obesity can be hard to treat with diet and exercise alone, so health care professionals may recommend weight-loss surgery. For people with a BMI of 30-35 who have type 2 diabetes that is difficult to control with medications and lifestyle changes, weight-loss surgery may be considered as a treatment option.
Calculate your BMI to learn whether you have obesity.
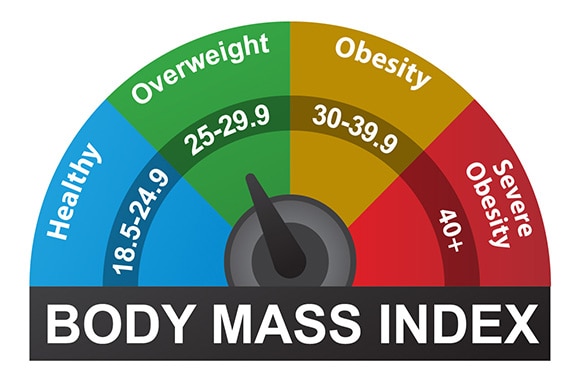 The BMI scale measures body fat based on weight in relation to height.
The BMI scale measures body fat based on weight in relation to height.Weight-loss surgery also may be an option to consider if you have serious health problems related to obesity, such as type 2 diabetes or sleep apnea. Weight-loss surgery can improve many of the medical conditions linked to obesity, especially type 2 diabetes.1,2
Does weight-loss surgery always work?
Studies show that many people who have weight-loss surgery lose on average 15 to 30 percent of their starting weight, depending on the type of surgery they have.3 However, no method, including surgery, is sure to produce and maintain weight loss. Some people who have weight-loss surgery may not lose as much as they hoped. Over time, some people regain a portion of the weight they lost. The amount of weight people regain may vary. Factors that affect weight regain may include a person’s weight before surgery, the type of operation, and adherence to changes in exercise and eating.
Weight-loss surgery can make it easier for you to eat fewer calories and be more physically active. Choosing healthy foods and beverages before and after the surgery may help you lose more weight and keep it off over the long term. Regular physical activity after surgery also helps keep the weight off. To improve your health, you must commit to a lifetime of healthy lifestyle habits and follow the advice of your health care professionals.
How much does weight-loss surgery cost?
Weight-loss surgery can cost between $15,000 and $25,000 or even more, depending on what type of surgery you have and whether you have surgery-related complications.4 Costs may be higher or lower depending on where you live. The amount your medical insurance will pay varies by state and insurance provider.
Medicare and some Medicaid programs may cover the major types of weight-loss surgery if you have a health care professional’s recommendation and you meet certain criteria (for example, if you have a BMI of 35 or greater and obesity-related health problems). Some insurance plans may require you to use approved surgeons and facilities. Some insurers also require you to show that you were unable to lose weight by completing a nonsurgical weight-loss program or that you meet other requirements.
Your health insurance company or your regional Medicare or Medicaid office will have more information about weight-loss surgery coverage, options, and requirements.
References
Types of Weight-loss Surgery
In this section:
- What are the surgical options?
- How is the surgery performed?
- What should I expect before surgery?
- What should I expect after surgery?
- How much weight can I expect to lose?
The type of weight-loss surgery, also called metabolic and bariatric surgery, that may be best to help a person lose weight depends on a number of factors. You should discuss with your doctor what kind of surgery might be best for you.
What are the surgical options?
In the United States, surgeons most often perform three types of operations
- gastric sleeve
- gastric bypass
- adjustable gastric band
Surgeons less commonly use a fourth operation, biliopancreatic diversion with duodenal switch.
Gastric sleeve
In gastric sleeve surgery, also called vertical sleeve gastrectomy, a surgeon removes most of your stomach, leaving only a banana-shaped section that is closed with staples. The surgery reduces the amount of food that can fit in your stomach, making you feel full sooner. Taking out part of your stomach may also affect hormones or bacteria in the gastrointestinal system that affect appetite and metabolism. This type of surgery cannot be reversed because some of the stomach is permanently removed.
Gastric bypass
Gastric bypass surgery, also called Roux-en-Y gastric bypass, is done in three steps. First, the surgeon staples your stomach, creating a small pouch in the upper section. The staples make your stomach much smaller, so you eat less because you feel full sooner.
Next, the surgeon divides your small intestine into two parts and attaches the lower part directly to the small stomach pouch. Food will bypass most of your stomach and the upper part of your small intestine, so your body absorbs fewer calories.
The surgeon then reconnects the upper part of the small intestine to a new location farther down on the lower part of the small intestine. This allows digestive juices in the stomach to flow from the bypassed part of the small intestine to the lower part of the small intestine, so that food can be fully digested. The bypass changes hormones, bacteria, and other substances in the gastrointestinal tract that may affect appetite and metabolism. Gastric bypass is difficult to reverse, although a surgeon may do it if medically necessary.
Adjustable gastric band
In this type of surgery, the surgeon places a ring with an inner inflatable band around the top of your stomach to create a small pouch. Like gastric sleeve and gastric bypass surgery, the gastric band makes you feel full after eating a small amount of food. The inner band has a circular balloon inside that is filled with saline solution. The surgeon can adjust the inner band to resize the opening from the pouch to the rest of your stomach by injecting or removing the saline solution through a small device, called a port, that is placed under your skin.
After surgery, you will need several follow-up visits to adjust the size of the band opening. If the band causes problems or is not helping you lose enough weight, the surgeon may remove it.
Today, adjustable gastric band surgery is less commonly performed in the United States, compared with the gastric sleeve or gastric bypass, because it is associated with more complications, predominantly the need for band removal due to intolerance.5 Gastric band surgery also typically results in significantly less weight loss and is associated with more complications, predominately the need for band removal due to intolerance.5
Biliopancreatic diversion with duodenal switch
A surgical procedure called biliopancreatic diversion with duodenal switch, or “mixed surgery,” involves two separate procedures. The first procedure is similar to gastric sleeve surgery. A second surgical procedure divides the small intestine into two tracts. Food moves through one tract, bypassing most of the small intestine. This reduces the number of calories and amount of nutrients absorbed. Digestive juices flow from the stomach through the other intestinal tract and mix with food as it enters the colon.
This type of surgery allows you to lose more weight compared with the other three operations described above. However, it is also the most likely to cause surgery-related problems and a shortage of vitamins, minerals, and proteins in your body. For these reasons, surgeons do not perform this particular procedure often. However, some surgeons may recommend it for patients who have severe obesity and certain health conditions.
Most Common Weight-loss Surgeries
Gastric Sleeve

What it is
A surgeon removes about 80 percent of stomach, creating a long, banana-shaped pouch.
Pros
- Greater weight loss than gastric band
- No changes to intestines
- No foreign objects placed in body
- Short hospital stay
Cons
- Cannot be reversed
- Risk of vitamin and iron deficiency (shortage)
- Higher chance of surgery-related problems than gastric band
- Risk of acid reflux and hiatal hernia (caused by the stomach pushing up against the diaphragm)
Gastric Bypass

What it is
A surgeon staples top part of the stomach, creating a small pouch, and attaches it to the middle part of the small intestine.
Pros
- Greater weight loss than gastric band
- No foreign objects placed in body
Cons
- Difficult to reverse
- Higher chance of vitamin and iron shortage than gastric band or gastric sleeve
- Higher chance of surgery-related problems than gastric band
- May increase risk of alcohol use disorder
Adjustable Gastric Band

What It Is
A surgeon places an inflatable band around top part of the stomach, creating a small pouch with an adjustable opening.
Pros
- Can be adjusted and reversed
- Short hospital stay and low risk of initial surgery-related problems
- No changes to intestines
- Lowest risk of vitamin shortage
Cons
- Less weight loss than other types of weight-loss surgery
- Frequent follow-up visits to adjust band; some people may not adapt to band
- Possible future surgery to remove or replace all or part of the band system.
Adapted from: Bariatric surgery procedures. American Society for Metabolic and Bariatric Surgery (ASMBS). Accessed October 5, 2020. https://asmbs.org/patients/bariatric-surgery-procedures. Image credit: Walter Pories, M.D., FACS.
How is the surgery performed?
Weight-loss surgery is mostly done laparoscopically, which requires only small cuts, under general anesthesia. Through these incisions, the surgeon can insert thin tools and a small scope attached to a camera that projects images onto a video monitor. Laparoscopic surgery has fewer risks than open surgery and may cause less pain and scarring. Recovery may also be faster with laparoscopic surgery.
Open surgery, which involves a single, large cut in the abdomen, may be a better option than laparoscopic surgery for certain people. You may need open surgery if you have a high level of obesity, had stomach surgery before, or have other complex medical problems.
What should I expect before surgery?
Before surgery, you will meet with several health care professionals, such as an internist, a dietitian, a psychiatrist or psychologist, and a bariatric surgeon.
- The internist will ask about your medical history, perform a thorough physical exam, and order blood tests. If you smoke, you may benefit from stopping smoking at least 6 weeks before your surgery.
- The dietitian will explain what and how much you will be able to eat and drink after surgery and help you prepare for how your life will change after surgery.
- The psychiatrist or psychologist may assess you to see if you are ready to manage the challenges of weight-loss surgery.
- The surgeon will tell you more about the surgery, including how to prepare for it and what type of follow-up you will need.
These health care professionals also will advise you to become more active and adopt a healthy eating plan before and after surgery. Losing weight and bringing your blood glucose—also known as blood sugar—levels closer to normal before surgery may lower your chances of having surgery-related problems.
Some weight-loss surgery programs have groups you can attend before and after surgery to help answer questions about the surgery and offer support.
What should I expect after surgery?
After surgery, you will need to rest and recover. Walking and moving around the house may help you recover more quickly. Start slowly and follow your health care professional’s advice about the type of physical activity you can do safely. As you feel more comfortable, add more physical activity.
After surgery, you will probably be started on a liquid diet. Over several weeks, you will move to a soft diet that includes such foods as cottage cheese, yogurt, or soup. Eventually you will begin consuming solid foods again. Your health care professional will tell you which foods and beverages you may have and which ones you should avoid. You will need to eat small meals and chew your food well. You will need to take dietary supplements that your health care professional prescribes to make sure you are getting enough vitamins and minerals.
How much weight can I expect to lose?
The number of pounds people lose after weight-loss surgery depends on the individual and on the type of surgery. One study found that after 1 year, people undergoing adjustable gastric banding, gastric sleeve, and gastric bypass lost between 38 and 87 pounds. Of the three most common procedures, gastric bypass produced greater weight loss, on average, but had more complications in the month after surgery. Most people regained some weight over time, but that amount was usually small compared with their initial weight loss.6
Your weight loss could be different. Remember, reaching your goal depends not only on the surgery but also on sticking with healthy lifestyle habits.
References
Weight-loss Surgery Benefits
What are the benefits of weight-loss surgery?
Weight-loss surgery, also called metabolic and bariatric surgery, can help you lose weight and improve many health problems related to obesity. These health problems include
- type 2 diabetes
- high blood pressure
- heart disease
- unhealthy cholesterol levels
- sleep apnea
- urinary incontinence
- knee, hip, or other body pain
For people with severe obesity, weight-loss surgery can extend years of life.7
You may be better able to move around and be physically active after surgery. You might also notice your mood improve and feel like your quality of life is better. As an added benefit, you may be able to take fewer prescription medications as you move into a healthier weight, which can reduce the cost burden.8

References
Weight-loss Surgery Side Effects
What are the side effects of bariatric surgery?
Side effects of weight-loss surgery, also called metabolic and bariatric surgery, may include
- bleeding
- infection
- leaking from the site where the sections of the stomach, small intestine, or both are stapled or sewn together
- diarrhea
- blood clots in the legs that can move to the lungs or heart
Follow-up interventions, surgery, and hospitalizations are relatively common within 5 years of weight-loss surgery, affecting about one-third of patients. Follow-up procedures are required more frequently after gastric bypass compared with gastric sleeve.9
Rarely, surgery-related problems can lead to death.
Other side effects may occur later. Your body may not absorb enough nutrients, especially if you don’t take your prescribed vitamins and minerals. Not getting enough nutrients can cause health problems, such as anemia and osteoporosis. Gallstones can occur after rapid weight loss. Some health care professionals prescribe medicine for about 6 months after surgery to help prevent gallstones. Gastric bands can move out of position or erode into the stomach wall and need to be removed.

Other problems that could occur later include strictures and hernias. Strictures—narrowing of the new stomach or the connection between the stomach and small intestine—make it hard to eat solid food and can cause nausea, vomiting, and trouble swallowing. Health care professionals treat strictures with special instruments to expand the narrowing. Two kinds of hernias may occur after weight-loss surgery—at the incision site or in the abdomen. Hernias can be repaired with surgery.
Some research suggests that weight-loss surgery, especially gastric bypass, may change the way your body absorbs and breaks down alcohol and may lead to more alcohol-related problems after surgery.
References
Potential Candidates for Weight-loss Surgery
Who is a good adult candidate for metabolic and bariatric surgery?
Weight-loss surgery, also called metabolic and bariatric surgery, may be an option for adults who have
- a body mass index (BMI) of 40 or more
- a BMI of 35 or more with a serious health problem linked to obesity, such as type 2 diabetes, heart disease, or sleep apnea
- a BMI of 30 or more with type 2 diabetes that is difficult to control with medical treatments and lifestyle changes
Having surgery to lose weight is a serious decision. If you are thinking about having weight-loss surgery, you should know what’s involved. Your answers to the following questions may help you decide if surgery is an option for you.
- Have you been unable to lose weight or keep it off using nonsurgical methods such as lifestyle changes or medication?
- Do you understand what the operation involves and its risks and benefits?
- Do you understand how your eating and physical activity patterns will need to change after you have surgery?
- Can you commit to following lifelong healthy eating and physical activity habits, medical follow-up, and the need to take extra vitamins and minerals?
- Have you considered the costs of the surgery and follow-up care?
Who is a good teen candidate for weight-loss surgery?
Health care professionals sometimes use weight-loss surgery to treat teens who have severe obesity and obesity-related health problems. Weight-loss surgery often improves health problems that could worsen in adulthood if the teen still has obesity.
Weight-loss surgery may be an option for teens as well. Guidelines10 recommend that teens be evaluated for surgery by a multidisciplinary team with expertise in pediatrics and have
- a BMI of 40
- a BMI of 35 or more with serious obesity-related health problems, such as type 2 diabetes or severe sleep apnea

Like adults, teens who are thinking about weight-loss surgery should be prepared for the lifestyle changes they will need to make after the surgery. A surgical center that focuses on the unique needs of youth may help the teen patient prepare for and adjust to these changes. Parents and caregivers also should be prepared and ready to support their child.
References
Clinical Trials
The NIDDK conducts and supports clinical trials in many diseases and conditions, including obesity. The trials look to find new ways to prevent, detect, or treat disease and improve quality of life.
What are clinical trials for weight-loss surgery?
Clinical trials—and other types of clinical studies—are part of medical research and involve people like you. When you volunteer to take part in a clinical study, you help doctors and researchers learn more about disease and improve health care for people in the future.
Researchers are studying many aspects of weight-loss surgery, also called metabolic and bariatric surgery, as a treatment for obesity, such as
- which types of weight-loss surgery might be appropriate for people who have severe obesity (BMI greater than or equal to 40) or lower levels of obesity (BMI less than 35)
- the effects of weight-loss surgery on conditions that frequently co-occur with obesity, such as diabetes
- interventions that can help weight-loss surgery patients maintain weight loss over time
Find out if clinical studies are right for you.
Watch a video of NIDDK Director Dr. Griffin P. Rodgers explaining the importance of participating in clinical trials.
What clinical studies for weight-loss surgery are looking for participants?
You can view a filtered list of clinical studies on weight-loss surgery that are federally funded, open, and recruiting at ClinicalTrials.gov. You can expand or narrow the list to include clinical studies from industry, universities, and individuals; however, the National Institutes of Health does not review these studies and cannot ensure they are safe. Always talk with your health care provider before you participate in a clinical study.
What have we learned about weight-loss surgery from NIDDK-funded research?
Longitudinal Assessment of Bariatric Surgery
From 2003 to 2016, the NIDDK partnered with researchers to create the Longitudinal Assessment of Bariatric Surgery, or LABS. The researchers examined the safety and effectiveness of two types of weight-loss surgery in adults, gastric bypass and adjustable gastric band.
LABS found that weight-loss surgery performed by experienced surgeons is relatively safe, leads to significant weight loss, and improves many weight-related health problems. After 7 years, the average weight loss of the gastric bypass patients was 84 pounds, or about 28 percent of their starting weight. The average weight loss of the gastric band patients was 41 pounds, or about 15 percent of their starting weight.12 In a separate analysis, LABS found that gastric band surgery was associated with a small but significant increased risk of problem alcohol use after surgery.13
Teen LABS
A separate group of researchers conducted similar research with teens in the severe obesity range and had serious weight-related health problems. This project, called Teen-LABS, found that at 5 years after the operation, patients who had gastric bypass surgery lost between 51 and 64 pounds.14 This represented about 26 percent of their starting weight. The teens also had improved overall health and quality of life. The Teen-LABS study is continuing for several more years, to gain information on the longer-term benefits and risks of weight-loss surgery with teens.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Anita P. Courcoulas, M.D., University of Pittsburgh, and Thomas Inge, M.D. Ph.D., Children’s Hospital of Colorado