

Hemodialysis
In this section:
- What happens during hemodialysis?
- Where can I have hemodialysis?
- How do I prepare for hemodialysis?
- What changes will I have to make when I start hemodialysis?
- How will I know if my hemodialysis is working?
- What are possible problems from hemodialysis?
- What happens if I have been on dialysis and I decide to stop?
Hemodialysis is a treatment to filter wastes and water from your blood, as your kidneys did when they were healthy. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood.
Hemodialysis can help you feel better and live longer, but it’s not a cure for kidney failure.
What happens during hemodialysis?
During hemodialysis, your blood goes through a filter, called a dialyzer, outside your body. A dialyzer is sometimes called an “artificial kidney.”
At the start of a hemodialysis treatment, a dialysis nurse or technician places two needles into your arm. You may prefer to put in your own needles after you’re trained by your health care team. A numbing cream or spray can be used if placing the needles bothers you. Each needle is attached to a soft tube connected to the dialysis machine.
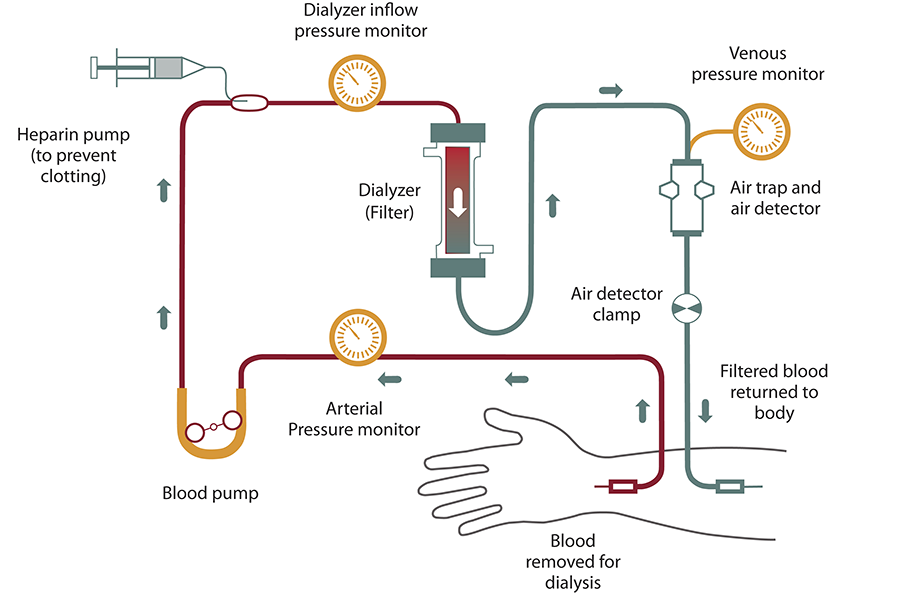
The dialysis machine pumps blood through the filter and returns the blood to your body. During the process, the dialysis machine checks your blood pressure and controls how quickly
- blood flows through the filter
- fluid is removed from your body
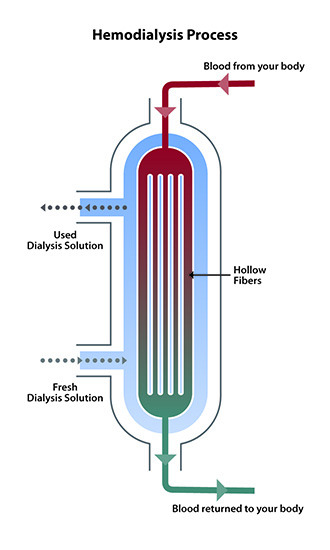
What happens to my blood while it’s in the filter?
Blood enters at one end of the filter and is forced into many, very thin, hollow fibers. As your blood passes through the hollow fibers, dialysis solution passes in the opposite direction on the outside of the fibers. Waste products from your blood move into the dialysis solution. Filtered blood remains in the hollow fibers and returns to your body.
Your nephrologist—a doctor who specializes in kidney problems—will prescribe a dialysis solution to meet your needs. The dialysis solution contains water and chemicals that are added to safely remove wastes, extra salt, and fluid from your blood. Your doctor can adjust the balance of chemicals in the solution if
- your blood tests show your blood has too much or too little of certain minerals, such as potassium or calcium
- you have problems such as low blood pressure or muscle cramps during dialysis
Can the dialyzer do everything my kidneys once did?
No. Hemodialysis can replace part, but not all, of your kidney function. Dialysis will help improve your energy level, and changes you make to your diet can help you feel better. Limiting how much water and other liquid you drink and take in through foods can help keep too much fluid from building up in your body between treatments. Medicines also help you maintain your health while on dialysis.
Where can I have hemodialysis?
You can receive treatment at a dialysis center or at home. Each location has its pros and cons.
Dialysis center
Most people go to a dialysis center for treatment. At the dialysis center, health care professionals set up and help you connect to the dialysis machine. A team of health care workers will be available to help you. You will continue to see your doctor. Other team members may include nurses, health care technicians, a dietitian, and a social worker.
Set schedule
You’ll have a fixed time slot for your treatments, usually three times per week: Monday, Wednesday, and Friday; or Tuesday, Thursday, and Saturday. Each dialysis session lasts about 4 hours. When choosing a dialysis schedule, think about your work and child care or other caregiving duties.
Nighttime option
Some dialysis centers offer nighttime treatments. These treatments occur at the dialysis center 3 nights a week while you sleep, which takes longer. Getting longer overnight dialysis treatments means
- your days are free.
- you have fewer diet changes.
- your liquid allowance (how much liquid you can drink) is closer to normal.
- you may have a better quality of life than with a standard hemodialysis schedule. Longer treatment sessions may reduce your symptoms.
How do I find a dialysis center?
Your doctor, nurse, or social worker can help you find a dialysis center that’s convenient for you. Under Medicare rules, you have the right to choose the dialysis center where you’ll receive treatment. You may want to use Dialysis Facility Compare, which rates all dialysis centers according to quality. Your doctor will give your medical information to the dialysis center you choose.
Most large cities have more than one dialysis center to choose from. You can visit the centers to see which one best fits your needs. For example, you can ask about a center’s rules for laptop and cellphone use, as well as for having visitors. You may want the center to be close to your home to save travel time. If you live in a rural area, the closest dialysis center may be far from your home. If you’d have a hard time getting to the dialysis center, you may want to consider home dialysis treatments such as home hemodialysis or peritoneal dialysis.
Home hemodialysis
Home hemodialysis lets you have longer or more frequent dialysis, which comes closer to replacing the work healthy kidneys do—usually three to seven times per week, and with treatment sessions that last between 2 and 10 hours. Machines for home use are small enough to sit on an end table.
If you choose to have your treatments at home, you’ll still see your doctor once per month.
Flexible schedule
You can choose a schedule that fits the way you live. You can use
- standard home hemodialysis—three times a week or every other day for 3 to 5 hours
- short daily hemodialysis—5 to 7 days per week for 2 to 4 hours at a time
- nightly home hemodialysis—three to six times per week while you sleep
Your doctor will decide how many treatments you need each week for daily or nightly home hemodialysis.
More dialysis filters your blood more thoroughly
Compared with a standard hemodialysis schedule, daily or nightly home hemodialysis will let you
- eat and drink more normally
- take fewer blood pressure medicines
Healthy kidneys work 24 hours a day, 7 days a week. Getting more hemodialysis feels more like having healthy kidneys and lowers your chances for problems that are common with a standard hemodialysis schedule, such as
- painful muscle cramps from removing too much fluid too quickly
- high blood pressure, which can cause a headache or, in rare cases, a stroke
- low blood pressure, which can make you faint, feel sick to your stomach, or be more likely to fall
- high phosphate levels, which can weaken bones and make your skin itch
Better quality of life
Standard hemodialysis can make you feel tired or washed out for several hours after each treatment. People who have switched from standard hemodialysis to longer or more frequent hemodialysis report they feel better, with more energy, less nausea, and better sleep. They also may report a better quality of life.1
Training for home hemodialysis
Most dialysis centers require that you have a trained partner in your home during hemodialysis treatments, so you must ask a family member or friend to go through the training with you. The clinic’s home-training nurse will teach you important safety skills.
During training, you and your care partner will learn to
- set up the machine
- take steps to prevent infection
- place needles into the vascular access
- respond to any alarms from the machine
- check your weight, temperature, blood pressure, and pulse
- record treatment details for the clinic
- clean the machine
- throw out used supplies safely
- track used supplies and order new ones
Training may take 4½ to 6 hours, 5 days a week, for 3 to 8 weeks. If you already know how to place the needles into your access, training may take less time.

The home-training nurse will make sure that you and your partner feel confident and may visit your home to help with your first at-home treatment. In addition to providing training and a hemodialysis machine that stays in your home, the dialysis center also provides 24-hour support if you have a question or problem. Some programs also monitor treatments over the internet.
Dialysis center and home hemodialysis comparison
Use the following chart to help you choose between treatment in a dialysis center or at home.
| Dialysis Center and Home Hemodialysis Comparison Chart | ||
|---|---|---|
| Dialysis center | Home | |
| Schedule | Three treatments a week for about 4 hours. Monday, Wednesday, Friday; or Tuesday, Thursday, Saturday. | Flexible. Three to seven short or long treatments per week at times that work best for you. |
| Availability | Available in most communities; may require travel in some rural areas. | Becoming more widely available as smaller equipment is developed. |
| Machine/supplies | The clinic has the machine and supplies. | The machine and 2- to 4-weeks’ worth of supplies are in the home. You may need minor changes in your home to connect the machine to electricity and water. |
| Training | The clinic teaches about treatments, diet, liquids, medicines, lab tests, etc. | You and a partner must attend 3 to 8 weeks of home hemodialysis training. |
| Diet and liquids | Strict limits on liquids, phosphorus, sodium, and potassium intake. | Fewer limits on liquids or diet, based on the amount of hemodialysis and lab tests. |
| Level of freedom | Less freedom on treatment days. May feel washed out and tired for hours after each treatment. | More freedom because you set the treatment schedule to meet the total amount prescribed. Work and travel are much easier. |
| Amount of work | Center staff members do hemodialysis tasks. They can teach you to do some tasks. | You and your partner must set up, run, and clean the machine; check vital signs; track the treatments and send in forms; and order supplies. |
| Payment | Medicare and most other health plans cover three hemodialysis treatments a week. | Medicare covers three hemodialysis treatments a week and may cover more for medical reasons; other health plans may cover all hemodialysis treatments. |
How do I prepare for hemodialysis?
Dialysis is a complex treatment that takes time to understand. Because most people don’t feel sick until shortly before starting dialysis, you’ll likely still feel well when your doctor first talks to you about getting ready for dialysis. No one wants to start you on dialysis before you need it, but it takes time to prepare for dialysis.
Take care of the blood vessels in your arms
It’s important for you to protect the veins in your arm prior to starting dialysis. If you have kidney disease, remind health care providers to draw blood and insert IV lines only in veins below your wrist; for example, ask them to use a vein in the back of your hand. If an arm vein is damaged by an IV line or by repeated blood draws, that vein may not be able to be used for dialysis.
Vascular access surgery
One important step before starting hemodialysis treatment is having minor surgery to create a vascular access. Your vascular access will be your lifeline through which you’ll connect to the dialyzer. Dialysis moves blood through the filter at a high rate. Blood flow is very strong. The machine withdraws and returns almost a pint of blood to your body every minute. The access will be the place on your body where you insert needles to allow your blood to flow from and return to your body at a high rate during dialysis.
Three types of vascular access exist
- an arteriovenous (AV) fistula
- an AV graft
- a catheter
Work closely with your nephrologist and vascular surgeon—a surgeon who works with blood vessels—to make sure the access is in place in plenty of time. Healing may take several months. The goal is for your access to be ready for use when you are ready for dialysis.
Watch a video of a doctor explaining vascular access.
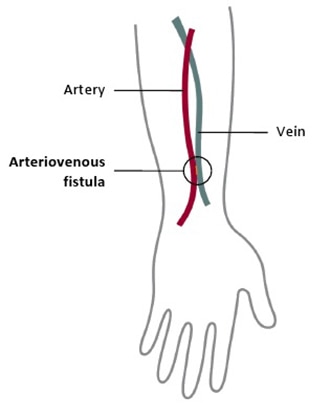
AV fistula
The best type of long-term access is an AV fistula. A surgeon connects an artery to a vein, usually in your arm, to create an AV fistula. An artery is a blood vessel that carries blood away from your heart. A vein is a blood vessel that carries blood back toward your heart. When the surgeon connects an artery to a vein, the vein grows wider and thicker, making it easier to place the needles for dialysis. The AV fistula also has a large diameter that allows your blood to flow out and back into your body quickly. The goal is to allow high blood flow so that the largest amount of blood can pass through the dialyzer.

The AV fistula is considered the best option because it
- provides highest blood flow for dialysis
- is less likely to become infected or clot
- lasts longer
Most people can go home after outpatient surgery. You will get local anesthesia to numb the area where the vascular surgeon creates the AV fistula. Depending on your situation, you may get general anesthesia and not be awake during the procedure.
Watch a video about why the fistula is the best access option.
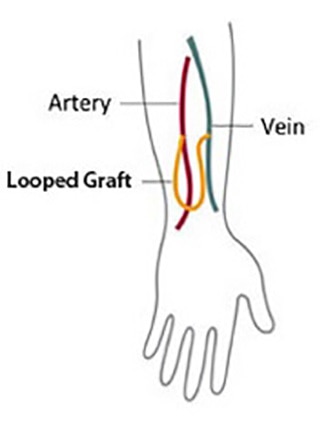
AV graft
If problems with your veins prevent you from having an AV fistula, you may need an AV graft instead. To create an AV graft, your surgeon uses a man-made tube to connect an artery to a vein. You can use an AV graft for dialysis soon after surgery. However, you’re more likely to have problems with infection and blood clots. Repeated blood clots can block the flow of blood through the graft and make it hard or impossible to have dialysis.
Catheter for temporary access
If your kidney disease has progressed quickly, or you have not had a vascular access placed before you need dialysis, you may need a venous catheter—a small, soft tube inserted into a vein in your neck, chest, or leg near the groin—as a temporary access. A nephrologist or an interventional radiologist—a doctor who uses medical imaging equipment to perform surgery—places the venous catheter while you’re in a hospital or at an outpatient clinic. You’ll receive local anesthesia and medicine to keep you calm and relaxed during the procedure.
Watch a video about problems with catheters.
What changes will I have to make when I start hemodialysis?
You have to adjust your life to build your dialysis treatment sessions into your routine. If you have in-center dialysis, you may need to rest after each treatment. Adjusting to the effects of kidney failure and the time you spend on dialysis can be hard. You may need to make changes in your work or home life, giving up some activities and responsibilities. Accepting these changes can be hard on you and your family. A mental health counselor or social worker can answer your questions and help you cope.
You will have to change what you eat and drink. Your health care team may adjust the medicines that you take.
Take care of your access
Your access is your lifeline. You will need to protect your access. Wash the area around your access with soap and warm water every day. Check the area for signs of infection, such as warmth or redness. When blood is flowing through your access and your access is working well, you can feel a vibration over the area. Let your dialysis center know if you can’t feel the vibration.
Make changes to what you eat and drink
If you’re on hemodialysis, you may need to limit
- sodium in foods and drinks.
- high-phosphorus foods.
- the amount of liquid you drink, including liquid found in foods. Fluid builds up in your body between hemodialysis treatments.
You may also need to
- add protein to your diet because hemodialysis removes protein
- choose foods with the right amount of potassium
- take vitamins made for people with kidney failure
- find healthy ways to add calories to your diet because you may not have a good appetite

Eating the right foods can help you feel better when you’re on hemodialysis. Talk with your dialysis center’s dietitian to find a hemodialysis meal plan that works for you.
How will I know if my hemodialysis is working?
You’ll know your hemodialysis treatments are working by how you feel. Your energy level may increase and you may have a better appetite. Hemodialysis reduces salt and fluid buildup, so you should have less shortness of breath and swelling as well.
This video explains how most people with kidney failure feel better after starting dialysis.
To make the most of your hemodialysis treatment, keep to your ideal “dry weight.” Your ideal dry weight is your weight when you don’t have extra fluid in your body. If you’re careful about the sodium in your diet and the hemodialysis is working, you should be able to reach your ideal dry weight at the end of every hemodialysis treatment. When hemodialysis treatments are working and you keep to your ideal dry weight, your blood pressure should be well controlled.

In addition, blood tests can show how well your hemodialysis treatments are working. Once a month, whether you’re on home or dialysis center hemodialysis, your dialysis center will test your blood. Read more about hemodialysis dose and adequacy.
What are possible problems from hemodialysis?
You could have a problem with your vascular access, which is the most common reason someone on hemodialysis needs to go to the hospital. Any type of vascular access may
- become infected
- have poor blood flow or blockage from a blood clot or scar
These problems can keep your treatments from working. You may need to have more procedures to replace or repair your access for it to work properly.
Sudden changes in your body’s water and chemical balance during treatment can cause additional problems, such as
- muscle cramps.
- a sudden drop in blood pressure, called hypotension. Hypotension can make you feel weak, dizzy, or sick to your stomach.
Your doctor can change your dialysis solution to help avoid these problems. The longer and more frequent treatments of home hemodialysis are less likely to cause muscle cramps or rapid changes in blood pressure than standard in-center dialysis.
You can lose blood if a needle comes out of your access or a tube comes out of the dialyzer. To prevent blood loss, dialysis machines have a blood leak detector that sets off an alarm. If this problem occurs at the clinic, a nurse or technician will be on hand to act. If you’re using home dialysis, your training will prepare you and your partner to fix the problem.
You may need a few months to adjust to hemodialysis. Always report problems to your health care team, who often can treat side effects quickly and easily. You can avoid many side effects by following an eating plan you develop with your dietitian, limiting liquid intake, and taking your medicines as directed.
What happens if I have been on dialysis and I decide to stop?
If you’ve been on dialysis and wish to stop, you’ll still receive supportive care. The dialysis social worker may be able to help you develop an end-of-life care plan before you stop dialysis.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Gayle Romancito, RN, Indian Health Service