

Solitary or Single-functioning Kidney
On this page:
- What is a solitary kidney?
- What causes a solitary kidney?
- How common is a solitary kidney?
- Who is more likely to have a solitary kidney?
- What are the complications of a solitary kidney?
- What are the symptoms of a solitary kidney?
- How do health care professionals diagnose a solitary kidney?
- How do health care professionals treat a solitary kidney?
- Can I prevent injury to my solitary kidney?
- How does eating, diet, and nutrition affect a solitary kidney?
What is a solitary kidney?
If you have only one kidney, that kidney is called a solitary kidney. This condition is different from having a solitary functioning kidney, in which you have two kidneys and only one is functioning.
What causes a solitary kidney?
The three main causes of a solitary kidney are:
Birth defects
Some people are born with only one kidney because the other kidney never developed—a condition known as renal agenesis or kidney agenesis. A solitary kidney is sometimes diagnosed before birth by a routine prenatal ultrasound; sometimes it is diagnosed later in life after an x-ray, an ultrasound, or a surgery for an unrelated clinical condition.
Some people are born with one normal kidney and another abnormal, nonfunctioning kidney that may eventually shrink so it is no longer visible on x-ray or ultrasound before or sometime after birth. That condition is known as kidney dysplasia.
Surgical removal of a kidney
Some people must have a kidney removed to treat kidney cancer or another disease or injury. That surgery is known as a nephrectomy. When a kidney is removed surgically, the ureter is also removed.
Kidney donation
A growing number of people are donating a kidney to be transplanted into a family member or friend whose kidneys have failed. Many people even donate a kidney to a stranger in need.
View full-sized image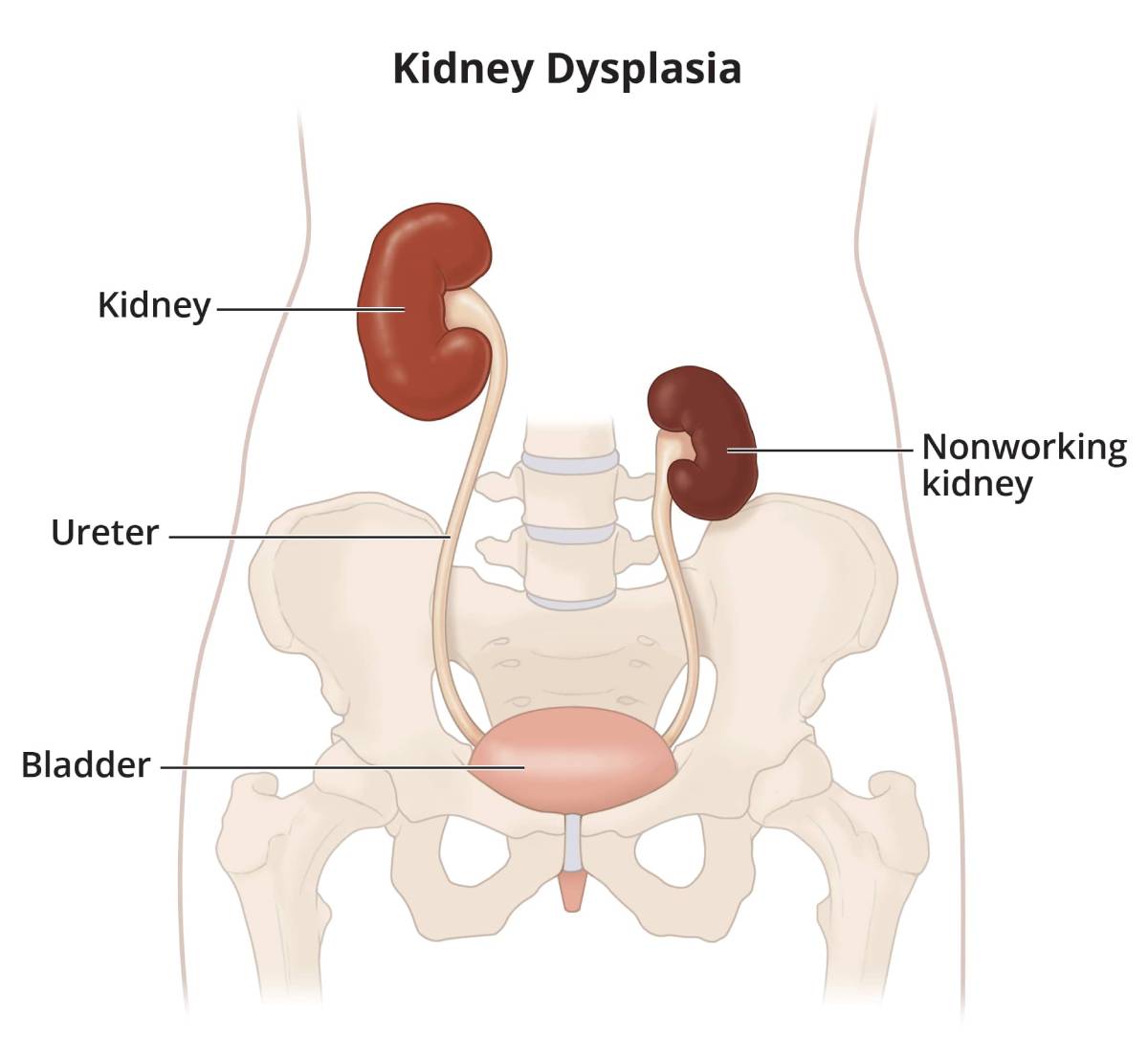 Some people are born with two kidneys, but one does not function, called kidney dysplasia.
View full-sized image
Some people are born with two kidneys, but one does not function, called kidney dysplasia.
View full-sized image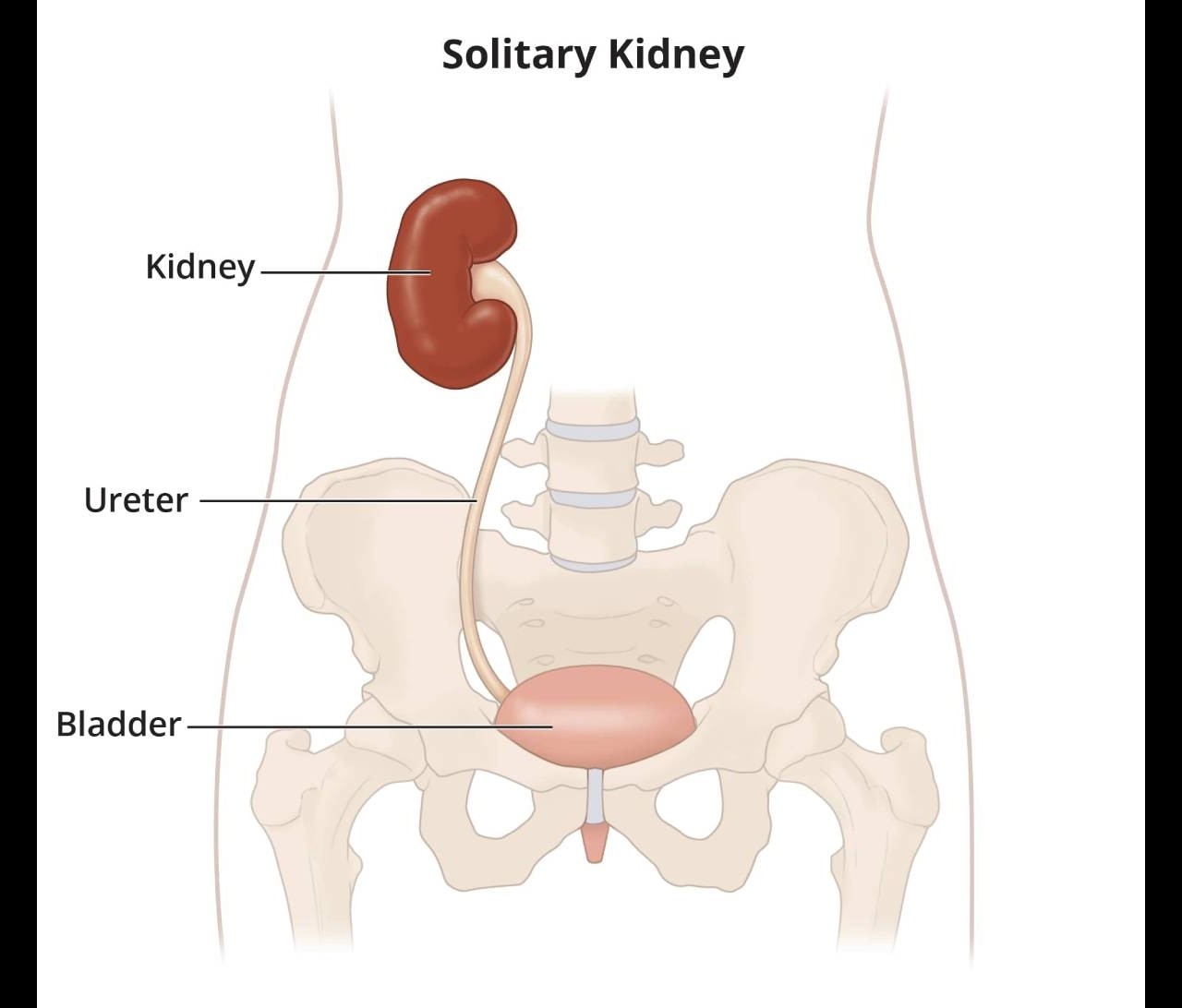 Some people are born with one kidney, called kidney agenesis, or have a kidney and ureter removed due to disease or for donation, called a solitary kidney.
Some people are born with one kidney, called kidney agenesis, or have a kidney and ureter removed due to disease or for donation, called a solitary kidney.
How common is a solitary kidney?
Globally, an estimated 1 in 2,000 babies1 are born each year with kidney agenesis and between 1 in 1,000 and 1 in 4,300 babies are born with kidney dysplasia. The estimates are probably low because some babies are never diagnosed with these conditions, particularly in countries where pregnant women do not routinely undergo prenatal ultrasounds.
Between 2008 and 2017, more than 58,000 Americans gave a kidney2 as living donors and more than 255,000 people had a kidney surgically removed to treat cancer,3 leaving them with solitary kidneys.
Who is more likely to have a solitary kidney?
Men are more likely than women to be born with a solitary kidney and to receive donated kidneys. Women, however, are more likely than men to be living kidney donors.3
What are the complications of a solitary kidney?
Complications from a solitary kidney are rare but may include
- increased protein in the urine, known as albuminuria.
- a lower-than-normal glomerular filtration rate (GFR), which measures how quickly your kidneys filter wastes and extra fluid from your blood. While less common, this complication can at times lead to kidney failure.
- high blood pressure.
- high blood pressure during pregnancy. This complication less commonly results in organ damage in the mother or child, a condition known as preeclampsia.
People with kidney agenesis or kidney dysplasia can be at an increased risk for developing kidney disease. For example, if your solitary kidney functioned normally during childhood, you still have an increased risk of having decreased kidney function as an adult.4,5
What are the symptoms of solitary kidney?
In general, people born with kidney agenesis or kidney dysplasia show no symptoms, lead full healthy lives, and may never discover they have a solitary kidney. Some people discover they have a solitary kidney by chance after having an x-ray, an ultrasound, or surgery for an unrelated condition or injury. A minority of people develop progressive loss of kidney function, and they can develop symptoms associated with chronic kidney disease.
A small percentage of babies born with kidney agenesis have other birth defects, such as an absent anus, an absent or smaller-than-normal bladder, an absent or smaller-than-normal uterus, a smaller-than-normal lung, club feet, or a hole in the heart wall separating the two lower heart chambers.5
How do health care professionals diagnose a solitary kidney?
During pregnancy, a health care professional can diagnose kidney agenesis and kidney dysplasia while conducting a prenatal ultrasound. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off the fetus’s organs to create an image of their structure. Ultrasounds during pregnancy are part of routine prenatal testing.
If a fetus is diagnosed with kidney agenesis or kidney dysplasia, health care professionals may recommend additional ultrasounds before and after the birth to find out how the solitary kidney functions over time and to check for other health problems.
In an adult, health care professionals may diagnose a solitary kidney during an x-ray, ultrasound, or surgery for some other condition or injury.
How do health care professionals treat a solitary kidney?
If you have a solitary kidney, your health care professional will
- monitor your kidney function by conducting urine and, sometimes, blood tests
- monitor and control your blood pressure
Testing your blood and urine
A health care professional uses two types of tests to monitor your kidney function
- a blood test that checks how well your kidneys are filtering your blood, called the glomerular filtration rate (GFR)
- a urine test to check for albumin, a protein that can pass into the urine when the kidneys are damaged
In some cases, your health care professional may perform additional tests to measure your kidney function.
 Blood and urine tests will help your health care professional monitor your kidney function.
Blood and urine tests will help your health care professional monitor your kidney function.
Monitoring and controlling your blood pressure
High blood pressure can damage blood vessels in your solitary kidney. If your kidneys’ blood vessels are damaged, they may no longer work properly. When this happens, the kidney is not able to remove all wastes and extra fluid from your body. Extra fluid in the blood vessels can raise your blood pressure even more, creating a dangerous cycle, and cause more damage leading to kidney failure.
If your health care professional diagnoses you with high blood pressure, he or she may prescribe one or more blood pressure-lowering medicines. Medicines that lower blood pressure can also significantly slow the progression of kidney disease.
Two types of blood pressure-lowering medicines, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), may be effective in slowing your kidney disease progression while also lowering your blood pressure. A health care professional may also prescribe a diuretic.
 Monitoring and controlling your blood pressure is particularly important if you have a solitary kidney.
Monitoring and controlling your blood pressure is particularly important if you have a solitary kidney.
Can I prevent injury to my solitary kidney?
You should let your health care professional know if you have a solitary kidney to prevent injury from medicines or medical procedures. Certain sports may be more likely to injure the kidney. This risk is of particular concern with children, as they are more likely to play sports. Talk with your health care professional about the specific sport and ways to lessen the risk of injury. Loss of the remaining working kidney will result in the need for dialysis or a kidney transplant.
How does eating, diet, and nutrition affect a solitary kidney?
If you have a solitary kidney, you do not need to eat a special diet. However, you can keep your kidneys healthy by staying well hydrated, not taking too much salt, and not gaining excessive weight. If you have reduced kidney function, you may need to make changes to your diet to slow your kidney disease progression. Work with your health care professional or a registered dietitian to develop a meal plan that includes foods you enjoy eating while maintaining your kidney health.
For more information about recommended dietary changes, refer to the NIDDK health topics, Nutrition for Early Chronic Kidney Disease in Adults, Diet & Nutrition for Adults with Advanced Chronic Kidney Disease, Nutrition for Children with Chronic Kidney Disease, and Managing Chronic Kidney Disease.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Tej K. Mattoo, M.D., D.C.H., F.R.C.P., F.A.A.P., Wayne State University School of Medicine